Seismic Compliance Frequently Asked Questions
For questions or comments related to the seismic frequently asked questions, please email the Seismic Compliance Unit (SCU).
General Questions
1. Do I need to submit drawings with the Seismic Evaluation Report?
The submittal requirements for the seismic evaluation can be found in 2022 California Administrative Code, Chapter 6, Section 1.3, Seismic Evaluation and all subsections which follow. These provisions stipulate that certain drawings and plans are an integral part of the Seismic Evaluation Report. The evaluator shall use drawings, diagrams, and details to accurately present the information necessary to communicate evaluated conditions and details of the subject existing building system.
The graphical information can be presented and incorporated in the evaluation report.
PDF format is preferred, oversized documents that are too large to upload to eSP may be submitted using our Secure File Transfer (SFT) website, click to request an SFT link.
2. Which Acute Care Hospitals are designated as rural and small hospitals in Seismic Zone 3?
Rural & Small Hospitals in Seismic Zone 3
| Hospital Facility Name | Notes |
|---|---|
| Alta District Hospital | Peer Group 5 |
| Barton Memorial Hospital | |
| Biggs-Gridley Memorial Hospital | |
| Bloss Memorial District Hospital | |
| Central Valley General Hospital | Federal Designation |
| Chowchilla District Memorial Hospital | |
| Colusa Community Hospital | |
| Corcoran District Hospital | |
| Del Puerto Hospital | |
| Dos Palos Memorial Hospital | |
| Eastern Plumas District Hospital | |
| Glenn General Hospital | |
| Hanford Community Hospital | |
| Indian Valley Hospital | |
| John C. Fremont Hospital | |
| Kingsburg District Hospital | Peer Group 5 |
| Lassen Community Hospital | |
| Lindsay Hospital Medical Center | |
| Mark Twain St. Joseph′s Hospital | |
| Marshall Hospital | |
| Mayers Memorial Hospital | |
| Memorial Hospital, Exeter | Peer Group 7 |
| Mercy Medical Center, Mt. Shasta | |
| Modoc Medical Center | |
| Needles-Desert Community Hospital | |
| Oak Valley District Hospital | Peer Group 5 |
| Palo Verde Hospital | |
| Plumas District Hospital | |
| Sanger Hospital | Peer Group 5 |
| Selma District Hospital | |
| Seneca District Hospital | |
| Sierra Nevada Memorial Hospital | Federal Designation/ Peer Group 5 |
| Sierra Valley Community Hospital | |
| Sierra-Kings District Hospital | Peer Group 5 |
| Siskiyou General Hospital | |
| Sonora Community Hospital | Peer Group 5 |
| St. Elizabeth Community Hospital | |
| Surprise Valley Community Hospital | |
| Sutter Amador Hospital | |
| Tahoe Forest Hospital | |
| Trinity Hospital | |
| Tuolumne General Hospital |
3. Can a different format be used for the “Compliance Plan Schedule” than the one specified in the regulations if we add a space for the governing codes and the year of construction?
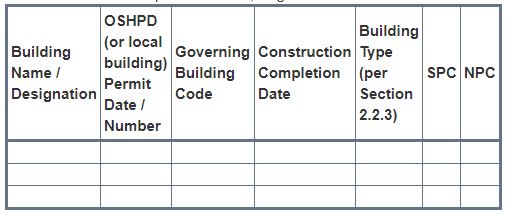
2022 California Administrative Code, Chapter 6, Section 1.4.4.4 specifies the items required for a complete “Compliance Plan Schedule” and Section 1.4.4.5 specifies the information required for the “Existing and Planned Buildings Matrix”. An augmented version of these documents is acceptable only if all the required items are included in the modified document.
4. We are doing a major SB 1953 retrofit on a hospital building. Will this trigger compliance with accessibility for disabled persons? Does the answer change if functional service areas are remodeled? Is there any range on cost to do accessibility changes?
Where the total cost of a retrofit, or remodel, exceeds the current valuation threshold discussed below, and the Office determines that the cost of full compliance is an unreasonable hardship, compliance shall be provided to the greatest extent possible; but in no case shall be cost of compliance be less than 20 percent of the cost of the alterations, structural repairs or addition. Where the total construction cost of a retrofit or remodel project does not exceed the most current valuation threshold and the cost of compliance with the accessibility requirements is disproportionate (i.e. exceeds 20% of the total project cost) without the required accessibility features, an “unreasonable hardship” may also exist. The Office will use the most current valuation threshold in determining if a retrofit or remodel project would create an “unreasonable hardship”. The 2021 valuation threshold is $172,418.00 and OSH-FD-800 application can be used when applicable.
The latest enforceable accessibility requirements for persons with disabilities contained in CBC Section 11B-202.4, Part 2, Title 24 (referenced from California Existing Building Code Section 305A.1) apply to any project submitted to the Office for hospital building retrofit or remodel, pursuant to SB 1953 regulations. HCAI/OSHPD does not have the authority to enforce federal (ADA) accessibility requirements for disabled persons. If functional service areas are remodeled, the remodeled area will also need to comply with any accessible elements and path-of-travel requirements associated with the specific area of remodel. For additional information refer to Code Application Notice (CAN) 2-11B.
5. Can a conforming hospital building (SPC 3, 4, 4D or 5) be supplied with utilities emanating from a SPC 1 hospital building?
A SPC 1 hospital building will cease operation as a general acute care hospital building at the end of the maximum extension granted to that building. Refer to California Existing Building Code Section 307A.1.1.1 for additions, alternations and remodels of conforming hospital buildings.
6. Which buildings fall under SB 1953, in cases where the building contains more than one licensed category of service?
Though a hospital building may provide different categories of services, HCAI is not aware of any hospital buildings which are licensed under multiple licensure categories. 2022 California Administrative Code, Chapter 6, Section 1.2, Definitions, has the term “General Acute Care Hospital” which specifies the types of buildings included under the auspices of SB 1953. This definition states in part that Hospital owners have various options under SB 1953 provisions for the continued use of noncompliant buildings. As part of the compliance plan, hospital owners may choose to remove all acute care services from selected buildings subject to the approval of the Department of Health Services Licensing and Certification Division (L&C).
7. If a Static Nonlinear (Pushover) design approach is used, can the hospital utilize the same engineering specialist that assists with the analysis to provide the peer review functions?
No, see 2022 California Building Code Section 1617A.1.41, Part 2, Title 24.
8. How do I add a hospital building to OSHPD’s building inventory, or certify an SPC 5/NPC 4 rating for a new building?
To add a building to OSHPD’s hospital inventory, or to certify a new building as SPC 5/NPC 4, submit a Seismic Compliance Project application using the eServices Portal (eSP), and upload the following supporting documents:
- Submit an Evaluation of the building per 2022 California Administrative Code (CAC), Chapter 6. If the building is a new OSHPD approved construction a letter stating that the building is conforming per 2022 CAC, Article 2.0.1 (Item 2.1) and Article 11.01.2 (Item 2) will suffice.
2022 California Administrative Code (CAC), Chapter 6
2022 CAC, Article 2.0.1, Item 2.1
A conforming building as defined in Article 1, Section 1.2, may be placed into SPC 5 in accordance with Table 2.5.3 under the following circumstances:
a. The building was designed and constructed to the 1989 or later edition of Part 2, Title 24, and
b. If any portion of the structure, except for the penthouse, is of steel moment resisting frame construction (Building, Type 3, or Building Type 4 or 6 with dual lateral system, as defined in Section 2.2.3) and the building permit was issued after October 25, 1994.
2022 CAC, Article 11.01.2, Item 2
The building is designated “NPC 4” in conformance with Table 11.1 “Nonstructural Performance Categories” and provided:
a. The building was designed and constructed under a building permit issued by HCAI, and
b. All subsequent repairs, remodels, additions and alterations were performed under a permit issued by HCAI, and
c. Fire sprinkler systems have been retrofitted in conformance with Table 11.1, “Nonstructural Performance Categories.”
Per Table 11.1, Fire sprinkler systems shall comply with the bracing and anchorage requirements of NFPA 13, 1994 edition, or subsequent applicable standards, effective date April 30, 1996 (Emergency Adoption).
- Include a Matrix of Construction per 2022 CAC, Chapter 6, Section 1.3.4, Item 6, page 86.
- Submit an amended or revised site plan showing the location of the building(s) to be added. We also recommend including approved drawings for this building (PDF format is preferred, oversized documents that are too large to upload to eSP may be submitted using our Secure File Transfer (SFT) website, click to request an SFT link). This will expedite the review as it takes time to retrieve the drawings from HCAI archives.
The SCU will assign SPC 5/NPC 4 to the building if the project under which the building was built is closed in compliance.
9. How do I remove Acute Care Services from a hospital building?
Please see eSP User Guide Applying for Removal of Acute Care Services. The 3-step process is summarized below;
Step 1: Submit a construction project using the eServices Portal (eSP)
If no construction is required for the removal of acute care services, this step may be skipped.
If construction is required to remove acute care services from a building submit one or more application(s) for new project to the Building Safety Section using the eServices Portal (eSP). See eSP User Guide Applying for Removal of Acute Care Services Section 3.1 for more information.
The project should demonstrate that the hospital building is eligible to have acute care services removed and that it can be transferred to either the local jurisdiction or remain in HCAI jurisdiction as a non-hospital building (this may include Acute Psychiatric or Skilled Nursing uses).
The 2022 California Existing Building Code, Section 312A outlines the requirements for such a project. Also see CAN 1-6-1.4.5.1.4 for examples on this issue, even though it has been superseded by the 2022 California Building Code. For further questions, contact the supervisor of the appropriate region of the Building Safety Section of HCAI/OSHPD where the building is located.
Step 2: Submit a no-construction project using the eServices Portal (eSP)
Once the construction project(s) from Step 1 have been completed and closed in compliance, submit a no-construction application for new project to the Building Safety Section using the eServices Portal (eSP). See eSP User Guide Applying for Removal of Acute Care Services Section 3.2 for more information.
Step 3: Submit a Removal of Acute Care Services (RACS) project to the Seismic Compliance Unit (SCU)
Once the no-construction RACS project from Step 2 has been completed and closed in compliance, submit a Seismic Compliance Project application using the eServices Portal (eSP), and upload the following supporting documents:
- Where HCAI jurisdiction is requested, provide the RACS project number and approval letter.
- Where Local jurisdiction is requested, provide the letter written by the supervisor of the appropriate region that hands the jurisdiction of the building to local authorities.
- Submit an amended or revised site plan showing the location of the buildings that remain in HCAI jurisdiction.
We also recommend including approved drawings for the RACS project (PDF format is preferred, oversized documents that are too large to upload to eSP may be submitted using our Secure File Transfer (SFT) website, click to request an SFT link). This will expedite the review as it takes time to retrieve the drawings from HCAI archives.
The SCU will then reclassify the building as OSHPD 1R and remove it from the list of buildings that need to comply with Senate Bill 1953. Where the building is being handed to local jurisdictions, the building is removed from the list of hospital buildings all together.
10. How are demolished buildings removed from the OSHPD building inventory?
Once the buildings have been demolished, submit a Seismic Compliance Project application using the eServices Portal (eSP), and upload the following supporting documents:
- Submit an amended or revised site plan showing the location of the remaining buildings.
- Submit relevant sheets of permit drawings under which the building was demolished (PDF format is preferred, oversized documents that are too large to upload to eSP may be submitted using our Secure File Transfer (SFT) website, click to request an SFT link).
- Submit a Field Staff Report showing start or completion of demolition or demolition progress photographs.
The SCU will then remove the building from the list of hospital buildings.
11. What is the Detailed Frame Joint Evaluation procedure for Pre-Northridge Moment Frame Buildings after an earthquake?
This is a 3-step process:
Step 1: Submit an application to the Seismic Compliance Unit (SCU)
Submit a Seismic Compliance Project application using the eServices Portal (eSP) for a Complete Joint Penetration (CJP) Joint Inspection Program per the 2022 California Administrative Code, Chapter 6, Section 4.2.0.3 where buildings have exceeded the ground motion specified in 2022 CAC Chapter 6, Section 4.2.0.1.
2022 California Administrative Code (CAC), Chapter 6
4.2 Steel moment frames. Welded steel moment frames may be subject to detailed frame joint evaluation requirements, as outlined in this section. The purpose of this joint evaluation is to determine if the building has experienced joint damage in strong ground shaking.
4.2.0.1 Preliminary screening. All welded steel moment frame structures shall undergo a detailed frame joint evaluation if the building is located at a site that has experienced the following:
1. An earthquake of magnitude greater than or equal to 6.5 that produced ground motion in excess of 0.20g; or
2. An earthquake that generated ground motion in excess of 0.30g.
The ground motion estimates shall be based on actual instrumental recordings in the vicinity of the building. When such ground motion records are not available, ground motion estimates may be based on empirical or analytical techniques. All ground motion estimates shall reflect the site-specific soil conditions.
4.2.0.2 Additional indicators. A detailed frame joint evaluation of the building shall be performed if any of the following apply:
1. Significant structural damage is observed in one or more welded steel moment frame structures located within 1 km of the building on sites with similar, or more firm, soil properties;
2. An earthquake having a magnitude of 6.5 or greater, where the structure is located within 5 km of the trace of a surface rupture or within the vertical projection of the rupture area when no surface rupture has occurred;
3. Significant architectural or structural damage has been observed in the building following an earthquake; or
4. Entry to the building has been limited by the building official because of earthquake damage, regardless of the type or nature of the damage.
4.2.0.3 Connection inspections. Detailed frame joint evaluations shall be performed in accordance with the procedures in the Interim Guidelines: Evaluation, Repair, Modification and Design of Welded Steel Moment Frame Structures, FEMA 267, August 1995.
Accessibility requirements for Detailed Frame Joint Evaluation Procedure for Pre-Northridge Moment Frame Buildings:
The detailed frame joint evaluation procedure for pre-Northridge moment frame buildings involves a visual, ultrasonic or magnetic particle inspection of moment frame joints in an existing building. As the inspections of the joint by itself does not constitute a “building alteration, structural repair or addition”, accessibility requirements of Chapter 11B of 2022 California Building Code do not apply. Spray-on-fireproofing or other fireproofing materials removed from the moment frame joint for the purposes of the inspection also do not constitute a “building alteration, structural repair or addition” where they are replaced in kind soon after the inspection (may be subject to special inspection under Section 1705A.14 Sprayed Fire-resistant materials). Where non-structural framing, finishes and/or ceiling systems are removed or altered temporarily to gain access to the joint, and then replaced in kind, the accessibility requirements apply only when the work performed exceeds an amount that would normally be required to gain access to the moment frame joint – a rule of thumb used in such cases is accessibility requirements apply when more than 25% of the ceiling in a room is temporarily removed/altered. Any repair, removal or alteration and replacement of structural systems such as beams, bearing and/or shear walls, will trigger accessibility requirements of Chapter 11B of the 2022 California Building Code, see examples in CAN 2-11B.
Step 2: Submit a construction project using the eServices Portal (eSP)
After the CJP Joint Inspection Program is approved, submit an application for new project to the Building Safety Section using the eServices Portal (eSP). Obtain a building permit and perform the joint inspection.
Step 3: Submit an application to the Seismic Compliance Unit (SCU)
Submit a Seismic Compliance Project application using the eServices Portal (eSP) for CJP Joint Inspection Results. If there is no damage, the SCU will concur with the results of the joint inspection and close the CJP Joint Inspection Program and Results projects.
Perform additional joint inspections depending on a damage index based on the results of field joint inspection where required. If damage is found, the SCU will discuss possible repair projects with the responsible design professionals.
Additional Notes:
- The joint inspections for affected buildings should be completed within six months after the earthquake.
- The joint inspection project should be left open until the SCU concurs with the results.
- Include notes on the process for inspection (2013 processforinspections.doc) with the joint inspection project.
- The joint inspection project will be reviewed by a fire marshal to verify replacement in kind of the fire proofing removed for the joint inspection.
12. Do buried tunnels have SPC or NPC ratings?
Buried tunnels connecting hospital buildings that are not used for public egress (such as utility tunnels with just service personnel access) receive NPC ratings only.
Buried Tunnels for public use (such as tunnels linking the basements of multiple hospital buildings) are required to have SPC and NPC ratings. The actual use of the tunnels may be verified by HCAI field staff.
Seismic Performance Category (SPC)
1. Can I submit a letter declaring the seismic performance category of a hospital building instead of a detailed Seismic Evaluation Report?
Per 2022 California Administrative Code, Sections 2.0.1.2 (SPC) and 11.01.2 (NPC) list the specific conditions where a hospital facility owner can submit a written declaration and be exempt from submitting either a structural or nonstructural evaluation report. However, the matrix of construction information specified in Section 1.3.4.6 shall be submitted pursuant to the requirements of Section 1.3.1. There are no other provisions for exemption from the Seismic Evaluation Report.
2. What if I don′t have any existing drawings?
When performing the structural evaluation for a hospital building without existing drawings or sufficient construction documents, as-built drawings as required by 2022 CAC, Chapter 6, Sections 2.1.2.1.1 and 2.1.2.2.2 shall be rendered to determine the SPC category of the specified hospital building. Refer to Sections 11.2.1.2, Item (d); 11.2.2, Item (e) and 11.2.3, Item (e), when performing the nonstructural evaluation to determine the NPC category of a hospital building without existing drawings or sufficient construction documents.
Additionally, the Seismic Evaluation Report and Compliance Plan/Schedule submittal process does not require original construction documents, only the information specified in Sections 1.3 and 1.4 and their respective subdivisions.
3. Is HCAI′s expectation that an SPC 2 upgrade provides a “Life Safety” level of performance?
The various levels of structural seismic performance established by SB 1953 include potential collapse hazard (SPC 1) to immediate occupancy (SPC 5) after a seismic event. The SPC 2 may not be repairable or functional after the event and, therefore; unable to provide general acute care hospital services. Buildings reclassified to SPC 2 on the basis of their collapse probability assessment (HAZUS) have a calculated probability of collapse which increases with the presence of significant structural deficiencies in the building.
4. Is HCAI′s expectation that an SPC 5 upgrade provides an “Immediate Occupancy” level of performance?
The various levels of seismic performance established by SB 1953 include potential collapse hazard (SPC 1) to immediate occupancy after a seismic event (SPC 5). The SPC 5 subgradation is currently the highest level of seismic structural performance. After a seismic event, it is anticipated that a SPC 5 facility will survive; suffering only very limited structural damage and will be able to provide full general acute care patient services (i.e. immediate occupancy).
5. How do I apply for an SPC 4D Material Testing and Condition Assessment Program (MTCAP) and Results (MTCAR) project?
The following steps explain the process for SPC 4D Material Testing and Condition Assessment Program and Results. However, the steps described below apply to any type of material testing projects (i.e. same for material testing required by SPC 2 “Usual Level” or SPC 4D “Comprehensive Level”).
Step 1: Submit an application to the Seismic Compliance Unit (SCU)
Submit a Seismic Compliance Project application using the eServices Portal (eSP) for SPC 4D Material Testing and Condition Assessment Program (MTCAP), and upload the following supporting documents:
- Submit complete MTCAP documents, detail drawings and specifications. Material Testing Program (MTP) and Condition Assessment Program (CAP) Programs can be submitted separately.
- The SCU will then review the structural scope of the MTCAP, the detail drawings and specifications. After the SCU approves the MTCAP the project will be closed. The SCU typically stamps the cover page of the report and sends the approved MTCAP report back to the Applicant.
Step 2: Submit a construction project using the eServices Portal (eSP)
Submit an application for new project to the Building Safety Section using the eServices Portal (eSP) and include the following:
- A copy of the SCU approved MTCAP Report and approval letter.
- Construction documents, which shall include all of the following:
- An overall building floor plan showing the proposed locations of inspection;
- Details and requirements for restoration of finishes and/or fire rated assemblies;
- When inspection impacts means-of-egress, a temporary exiting plan;
- Plans and details for temporary construction barriers;
- Fire watch procedures: When it is not possible to maintain fire-resistive assemblies, fire-resistive construction and/or the means of egress, temporary construction barriers and/or a fire watch shall be provided in accordance with HCAI/OSHPD PIN 14.
- Specifications
- TIO form
(These projects may be processed in accordance with the FREER Manual as a Field Review project)
HCAI/OSHPD region review includes architectural, structural, fire/life safety. Electrical or mechanical review are typically not required.
After the HCAI/OSHPD region approves the project and issues a permit for the MTCAP project, the construction phase (i.e. testing) begins.
During the Conditions Assessment, fire-resistive assemblies, fire-resistive construction and the means of egress shall be maintained in accordance with Chapters 7 and 33 of the California Fire Code. These plans and procedures shall be reviewed and approved by the HCAI field staff (Compliance Officer, Fire and Life Safety Officer and District Structural Engineer) and the local fire authority (as applicable) in accordance with Section 3301 of the 2022 California Fire Code. Compliance with the provisions of Chapter 33 of the 2022 California Fire Code are in addition to any additional regulations or requirements pertaining to dust control, noise control and asbestos abatement enforced by agencies other than HCAI/OSHPD.
When demolition, inspection and reconstruction is continuous, no hot work is involved and inspectors and construction workers are in constant attendance, enforcement of temporary construction barrier and / or fire watch requirements may be deferred. Under these conditions, appropriate procedures shall be established in the event of a fire or other emergency.
During sampling stage, if any deviation from the MTCAP report occurs, such as sampling location, number of samples etc., SCU shall be notified immediately via email with a brief description of the change, a photo and any additional supporting documentation. To prevent any construction delays, SCU will respond back via email as soon as possible (Keep track of these responses, as these communications will be required in the MTCAR report).
Where changes are extensive, an amended construction document may be required at the discretion of the District Structural Engineer in consultation with the SCU.
The SCU recommends that the project remain open (within time limitations per 2022 CAC 7-129) until the results are accepted by the SCU in case additional testing or inspection is required.
Step 3: Submit an application to the Seismic Compliance Unit (SCU)
Submit a Seismic Compliance Project application using the eServices Portal (eSP) for SPC 4D Material Testing and Condition Assessment Results (MTCAR), and upload the following supporting documents:
- Submit complete MTCAR reports, include all deviations, and corresponding SCU approval emails.
- The SCU will issue and MTCAR approval letter and close the project.
- Contact the Building Safety Section and request to close the construction project.
6. What ACI 318 version should be used in analysis/evaluation and construction drawings for the concrete detailing of new structural members in SPC-4D retrofit projects?
Seismic evaluation for SPC-4D compliance can be performed using ASCE 41-13 Chapter 17 reference standards or later version (ACI 318-11 or later version) as long it is consistent throughout the evaluation. However, per 2022 CEBC Section 302A.4, concrete detailing of new structural members and connections shall comply with the detailing provisions of the current California Building Code for new buildings of similar structure, purpose and location. Per current code 2022 CBC Chapter 35, concrete construction shall conform to the provisions of ACI 318-19.
7. What does “Not a Building Structure” on the HCAI website mean?
“Not a Building Structure” are buildings that are not intended for occupancy by people except for maintenance and other intermittent access and that are not constructed in the manner of a building. Examples of buildings that are classified as Not a Building Structures are:
- Cooling Towers
- Elevated platforms supporting equipment
- Fabricated bolted together enclosures such as emergency generator sound enclosures
- Tank structures
8. Can outside canopies be designed using ASCE 41-13 Chapter 13?
For outside on the ground, one story independent canopy steel structures, ASCE 41-13 Chapter 9 steel structure criteria under BSE-1E and BSE-2E shall be used. ASCE 41-13 Chapter 13 is not acceptable.
9. What are the requirements involving IOR participation in the extraction and passing of concrete core samples to the testing laboratory in a Material Testing and Condition Assessment Program?
The design professional of record shall discuss with OSHPD field staff prior to the implementation of the process below:
- The IOR should verify that, prior to coring, the reinforcement was scanned and located, that the core is located in an area that will not damage reinforcement, and that the core matches the location on the material testing plans.
- The IOR does not need to be present for the coring, but after the coring is complete, and prior to any infill/patching, the IOR should confirm that no reinforcement was cut/damaged.
- The above items fall under the IOR’s duties per CAC 7-145(a)1 and 2.
- The above inspection can be handled by a Class A or Class B IOR.
10. What is the SPC 4D evaluation requirement for penthouse structures?
Penthouse structures with aggregate area that is less than one-third of the roof area or is not an extension of the building frame can be evaluated using either criteria 1 or 2 listed below:
- ASCE 41-13 Chapter 13 criteria under BSE-1E. The connection to the existing structure shall be designed for amplified omega level (Ω=2) demands.
- ASCE 41-13 Chapter 13 criteria under BSE-2E.
Penthouse structures larger than one-third of the roof area and/or an extension of the building frame shall be evaluated using their respective material chapter for both BSE-1E and BSE-2E against Damage Control and Collapse Prevention respectively.
11. Does the CEBC Section 304A.3.5.12 regarding Concrete Shear Wall Coupling Beams apply to both shear and flexure? What are the criteria for reinforcing not similar to wall section?
Horizontal wall segment or spandrels controlled by shear action and reinforced similar to vertical wall segments or piers shall be classified as wall segments., not shear wall coupling beams, in ASCE 41-13 Table 10-20 and Table 10-22. Horizontal wall segments or spandrels with either closed hoops or stirrups anchored to the longitudinal reinforcing at the top and bottom with a standard hook may be classified as shear wall coupling beam. The requirement in this sentence “Horizontal wall segments or spandrels reinforced similar to vertical wall segments or piers shall be classified as wall segments, not shear wall coupling beams, in Tables 10-19 through 10-22.” does not apply to flexure controlled wall segments or spandrels.
12. Can the stiffness per ASCE 41-13 Table 10-5 of a coupling beam be lowered in evaluation?
Effective Stiffness Values of a coupling beam shall be based on ASCE 41-13 or equivalent provision in later version of the ASCE 41.
13. When is a shear-friction check required? The capacity provided in ACI 318 is limited to only steel strength crossing the potential crack. Is it possible to use other equations as referenced under the ACI 318 commentary?
ACI requires a shear-friction check across any given plane, such as an existing (cold joint) or potential crack. Shear friction shall be evaluated in the diaphragm slab to transfer the load to the wall in addition to the locations where the cold joint is clearly shown in construction documents. For the calculation of the strength of reinforced concrete interface, the following equations may be used in lieu of the ACI 318-19 equation 22.9.4.2 or equivalent versions of ACI 318 not to exceed table ACI 318-19 22.9.4.4 nor 2 times ACI 318-19 equation 22.9.4.2.
Normal weight vu = 0.8 ρfy + 400 psi
Sanded lightweight concrete vu = 0.8 ρfy + 250 psi
All-lightweight concrete vu = 0.8 ρfy + 200 psi
Deformation-controlled shear friction behavior is only permitted for cold joints located at the interface between walls and foundation per ACI 369.1-22 §7.4.1.
14. Clarification for application of ASCE 41-13 §7.2.8.1 related to overturning
For the evaluation of one-story light-framed walls with or without hold-downs, ASCE 41-13 equation 7-6 is permitted to be used. If equation 7-6 is satisfied, no further evaluation or retrofit of the existing hold-down, if any, is required. If equation 7-6 is not satisfied, hold-down shall be provided or retrofitted using ASCE 41-13 equations 7-36 and 7-37. Equation 7-6 shall not be used to limit forces to other elements. Other elements, such as the diaphragm, collector, shear wall, sill bolts, etc, shall be evaluated independently using ASCE 41-13 equations 7-36 and 7-37 with the associated m or J factors listed under Chapter 12. Alternatively, if equation 7-6 is not satisfied and retrofit is not performed, the wall contribution to the lateral resisting system shall be ignored.
For all other building type conditions, equation 7-6 shall not be used. If a shear wall is opened for retrofit, we strongly recommend adding holdowns to any shearwall that does not already have them.
15. What ASCE 41-13 parameters shall be used for flexurally controlled shear walls and wall segments with inadequate lap splices?
Flexurally controlled shear walls with inadequate lap splices shall be treated as force-controlled elements if Equation 10-1 yields an fₛ value less than fᵧₗ. If fₛ exceeds fᵧₗ, the wall may be treated as deformation controlled with Plastic Hinge Rotation parameters a and b, along with the Acceptable Plastic Hinge Rotation values specified in Table 10-19 in nonlinear analysis (The residual strength parameter c shall not exceed 0.20) and m-factors in Table 10-21 for linear analysis.
In both linear and non-linear analyses, the reinforcement strength shall be based on fₛ as determined in accordance with Section 10.3.5.
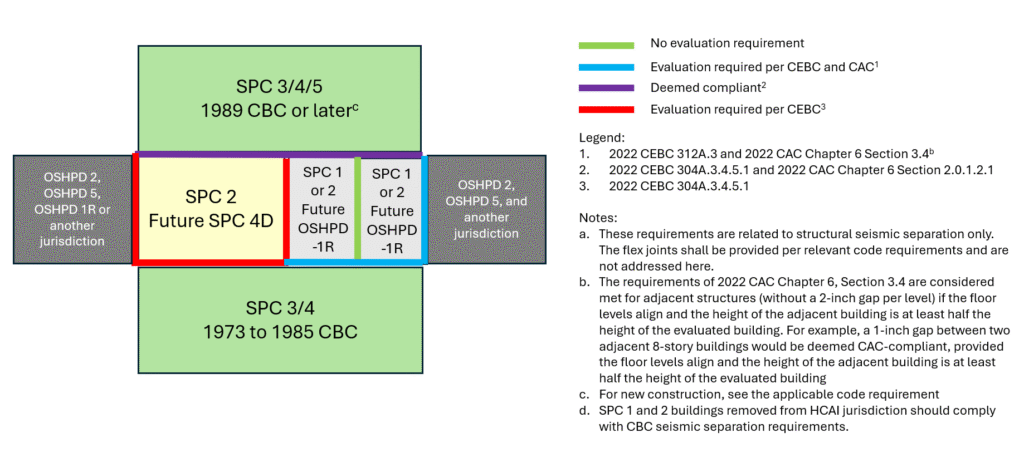
16. What are the requirements for evaluation seismic separations for SPC 1 or SPC 2 buildings undergoing RACS or SPC 4D upgrade?
17. What are the reinforcing requirements, acceptable performance criteria, and retrofit methods for reinforced masonry walls under SPC-4D regulations?
- Reinforcing Compliant with TMS Requirements
When reinforcing complies with TMS reinforced masonry requirements, both shear and flexure shall be considered deformation-controlled, and the use of ASCE 41 Tables 11-6 and 11-7 is permitted. - Reinforcing Not Compliant with TMS but Compliant with ASCE 41
When reinforcing does not comply with TMS reinforced masonry requirements but does comply with ASCE 41 reinforced masonry requirements (as defined below), shear actions shall be treated as force-controlled, while flexure shall remain deformation-controlled. The use of Tables 11-6 and 11-7 for flexure is permitted. Application of FRP for flexure is not permitted. - Vertical Reinforcing Compliant; Horizontal Reinforcing Not Compliant
If vertical reinforcing complies with ASCE 41 reinforced masonry requirements, but horizontal reinforcing does not, application of FRP for shear retrofit is permitted where FRP is applied on both sides of the 8” hollow unit reinforced masonry walls or 9” solid unit reinforced masonry wall. Application of FRP on one side is not permitted. FRP retrofit is not an acceptable solution for thicker walls. Shotcrete is permitted to be used to retrofit thicker walls. Flexure shall remain deformation-controlled. The use of Tables 11-6 and 11-7 for flexure is permitted. Application of FRP for flexure is not permitted. - Neither Vertical nor Horizontal Reinforcing Compliant
If neither vertical nor horizontal reinforcing complies with ASCE 41 reinforced masonry requirements, the wall element shall not be considered part of the lateral load-resisting system. FRP retrofit is not an acceptable solution. Shotcrete may be used to retrofit these walls.
ASCE 41 Reinforced Masonry : Masonry with the following minimum amounts of vertical and horizontal reinforcement: vertical reinforcement of at least 0.20in.2 in cross-section at each corner or end, at each side of each opening, and at a maximum spacing of 4 ft throughout. Horizontal reinforcement of at least 0.20 in.2 in cross-section at the top of the wall, at the top and bottom of wall openings, at structurally connected roof and floor openings, and at a maximum spacing of 10ft.
CEBC Section 2.3 UNREINFORCED MASONRY. [OSHPD 1, 1R, 2, 4 & 5] Unreinforced masonry as used in this chapter means masonry construction where reinforcements in any direction is less than minimum reinforcement specified in TMS 402 Section 7.3.2.6.
18. For an SPC 4D material testing project results conducted in accordance with ASCE 41-13, how should material strength values be determined for analysis when test results exhibit a coefficient of variation (COV) greater than 20% for concrete (or 25% for masonry)?
Higher COV might represent a concern with material quality and require further review. Dependent on each specific condition, and as approved by OSHPD, one of the following methods could be used:
- Additional tests shall be performed until the coefficient of variation is equal to or less than 20% for concrete (or 25% for masonry). Expected values and lower bound values are the mean and the mean minus one standard deviation, respectively.
- A knowledge factor of 0.75 as specified in ASCE 41-13 §10.2.4 and §11.2.4 shall be used in analysis. Expected values and lower bound values are the mean and the mean minus one standard deviation, respectively.
- A knowledge factor of 1 as specified in ASCE 41-13 may be used in analysis provided that in calculating capacity of elements, expected values and lower bound values are the mean minus one standard deviation. Where strength is used to determine demands based on maximum force that can be delivered to an element, such as column under discontinuous shear wall, higher expected values (mean) shall be used.
19. ASCE 41-13 does not address the inadequate bar development length in masonry buildings. What are the requirements for inadequate development in masonry buildings?
Steel Reinforcement Yield Strength Properties The expected yield strength of reinforcing bars, fye, shall be based on mill test data or on tension tests of actual reinforcing bars taken from the subject building. Where development lengths and lap splices of existing deformed bars meet the provisions of TMS 402, the yield strength does not need to be adjusted. Where development lengths and lap splices of existing deformed bars do not meet the TMS 402 requirements, the yield strength shall be adjusted using Equation (11-8):
fye = (lb∕ld) × fyE ≤ fyl/E
fyE = Expected strength of reinforcement from testing, lb/in.2
fyl/E = lower-bound or expected yield strength of reinforcement from testing, as applicable to force controlled or deformation-controlled actions, respectively, lb/in.2
If lb is less than 12 in. (305 mm), fye shall be taken as zero. If lb is less than 80% of ld, members shall be deemed to force controlled because of inadequate splicing. As an alternative, testing may be used to determine the lap splices can perform as deformation controlled.
For RM wall components, existing plain reinforcement development and lap splice lengths shall be taken as twice the values determined per TMS 402 for a deformed bar of equivalent diameter unless other lengths are justified by approved tests or calculations considering only the bond between the bar and the concrete. The allowed length shall not be less than the value for deformed bar per TMS 402.
20. What are the FRP retrofit requirements and acceptable performance criteria for SPC-4D for reinforced concrete walls and diaphragms?
Where an existing shear wall, wall segment, or diaphragm has a reinforcement percentage, ρₙ, in both the horizontal and vertical directions equal to or greater than 0.0015, shear may be assumed to be deformation-controlled. Table 10-20 of ASCE 41-13 with a maximum acceptable rotation of 1.5% at CP level may be used for nonlinear analysis. Table 10-22 of ASCE 41-13 with a maximum “m” value of 2.5 at CP level may be used for linear analysis.
Where an existing shear wall, wall segment, or diaphragm has a reinforcement percentage, ρₙ, in both the horizontal and vertical directions equal to or greater than 0.001 but less than 0.0015, shear shall be assumed to be force-controlled.
Where an existing shear wall or wall segment has a reinforcement percentage, ρₙ, less than 0.001 in either direction, the application of FRP is not allowed. Shotcrete may be used as an option for retrofit of these elements.
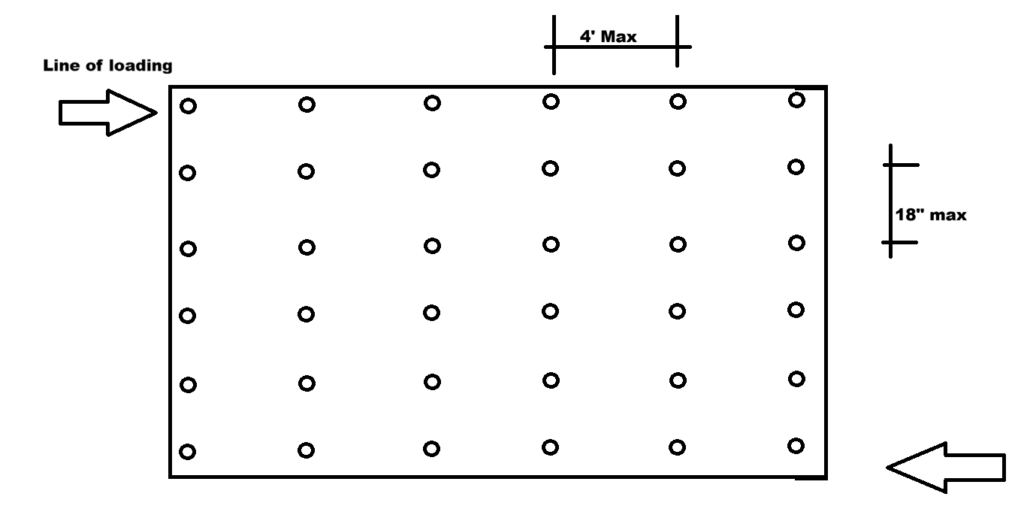
Anchors shall be provided in lines perpendicular to the line of loading, spaced at maximum 4 feet apart. The spacing of anchors in each line shall not exceed 18 inches. Anchor embedment shall be equal to the wall thickness minus 2 inches up to 6”.
One sided FRP is allowed for concrete thicknesses of 8 inches or less. For walls or diaphragms thicker than 8 inches, FRP shall be applied to both sides.
The maximum allowable design strain for shear strengthening shall be 0.0015 in/in. For design and other requirements, follow the manufacturer’s guidelines.
21. What are the FRP retrofit requirements and acceptable performance criteria for collectors and slab/wall or wall/foundation connections?
Both anchored and unanchored FRP may be used for collectors and for slab/wall or wall/foundation connections. The bonding capacity and anchor capacity shall not be combined. The shear friction including FRP action shall be considered force controlled.
FRP without anchors
For collectors, the maximum allowable design tensile strain for FRP without anchors is 0.0015 for maximum 0.12-inch thickness of FRP. Application of thicker FRP is not acceptable without anchor. For slab/wall or wall/foundation connections, the maximum capacity is 10 k/ft with minimum corner radius of 2.5” filled with FRP and epoxy per manufacturer guideline.
The minimum concrete–FRP bond strength for bond-critical applications and any required mechanical anchorage is 200 psi.
FRP with anchors
For collectors, the maximum allowable design tensile strain for FRP with anchors is 0.003. For slab/wall or wall/foundation connections, the maximum capacity is 15 k/ft.
The maximum spacing of anchors is 24 inches. In calculating the capacity of anchors, ACI limit states and FRP anchor shear capacity shall be considered.
For design and other requirements, follow the manufacturer’s guidelines.
Nonstructural Performance Category (NPC)
1. The continuous operation issue is to be addressed for hospitals that are to remain in existence beyond the 2030 deadline. Prior to 2030 deadline, why does the Nonstructural Performance Category (NPC) 3 category require components that are part of continuous operation systems to be anchored and braced, when located in critical care areas and other support areas critical to patient care?
The NPC′s were developed with the intent of establishing various levels of seismic performance for nonstructural equipment, components and systems critical to patient care. The critical distinction between any two NPC′s is not merely the survivability of the facility, but its level of functionality after a seismic event. Nonstructural components and systems have a lower threshold to seismic forces than structural elements and systems.
Buildings in the NPC 3 category are expected to maintain their inpatient population following a moderate earthquake, as well as provide a full array of emergency services to the public. To enable a NPC 3 hospital building to provide these level of services (i.e. beyond mere survivability and be able to provide a minimal amount of medical care in specific areas) it is necessary to provide the bracing and anchorage specified in California Administrative Code, Chapter 6, Table 11.1, Nonstructural Performance Categories.
2. Do critical care areas such as Emergency Rooms, which are not part of the required Basic Services, have to meet the requirements of NPC?
In 2022 CAC, Chapter 6 Section 1.2, Definitions, the term “Critical Care Area” is defined as “those special care units…in which patients are intended to be subjected to invasive procedures and connected to line-operated, electromedical devices.” Within this definition, “emergency rooms” is listed as a type of critical care area. The 2022 California Administrative Code, Chapter 6, Table 11.1 lists “Critical Care Areas” in NPC 3 as an area where specified components/equipment/systems must meet the bracing and anchorage requirements of Part 2, Title 24. Therefore, “emergency rooms” must meet the requirements as specified in the NPC 3.
3. Would a Neurocare Ward (not ICU) with patients hooked up to a ventilator fall under the definition of “critical care”? Also, would a telemetry unit be considered “critical care” area?
A neurocare ward would be considered a “critical care” area due to the nature of the treatment for the patients placed in them or the type of service provided (e.g. postoperative from brain surgery, etc.). A telemetry unit need only be considered for evaluation purposes if it supports a critical care area. In this context, a “telemetry unit” is defined as a group of patient beds with remote monitoring.
4. CAC 2022 Table 11.1 for NPC 4 says “and all architectural, mechanical, electrical systems, components and equipment”. Does this mean that the NPC 3 Exceptions do not apply? (i.e. seismic bracing for cable trays, conduits and HVAC are not excluded anymore)
NPC 4 includes all electrical, mechanical, architectural. So, if NPC 4 upgrade in a NPC 3 building is desired, NPC 3 exceptions items are also required to be braced and anchored per 2022 CAC Chapter 6 Table 11.1. In other words, all components and equipment are required to be anchored and braced per Part 2 Title 24 under NPC 4. Alternate path forward can be NPC 4D route, where you can follow NPC 3 exceptions.
5. One of our hospital buildings does not have fire sprinklers. If this building is seismically retrofitted to SPC 2 level, will this require us to install a fire sprinkler system? What if it is retrofitted to SPC 5 level?
Sprinkler systems fall under the Nonstructural Performance Categories (NPC′s) and not under the Structural Performance Category (SPC) requirements. Compliance with SB1953 does not require that fire sprinkler systems be installed where none existed before, even for SPC 5 conformance. However, hospital buildings with existing fire sprinkler systems must meet the anchorage and bracing requirements of NPC 3 and NPC 4.
6. Are there areas within a typical hospital where the Nonstructural Evaluation requirements of SB 1953 do not apply?
The answer to this question depends on the desired NPC level of performance. Table 11.1, Nonstructural Performance Categories, determines the applicability of the nonstructural evaluation requirements for a hospital. If the desired performance level is NPC 4 or 5 (for acute care operation beyond 2030) then all areas of the hospital are subject to the requirements as listed in California Administrative Code, Chapter 6, Table 11.1. However, NPCs 2, 3 and 4D primarily impact critical care areas of a hospital, with adjacent non-critical care areas affected by presence of specific systems (e.g. communications, emergency power, means of egress, fire alarm and med-gas) as delineated in California Administrative Code, Chapter 6, Table 11.1.
7. Are single line diagrams required for the location of certain hospital areas?
The Nonstructural Evaluation Report (see 2022 California Administrative Code, Chapter 6, Article 1, Section 1.3.4, Item 2.1) must include single line diagrams for the location of the following:
- Central supply areas
- Clinical laboratory service spaces
- Critical care areas
- Pharmaceutical service spaces
- Radiological service spaces
- Sterile supply areas
There are no provisions requiring single line diagrams for other hospital areas.
8. What is meant by “description…where deficiencies are identified” in Section 1.3.4, Item 2.2 of Article 1?
Nonstructural elements and systems which do not meet the requirements of Article 11 should be reported as deficiencies. These deficient systems/elements should be described in the nonstructural evaluation either in narrative or diagrammatic format as specified in 2022 California Administrative Code, Chapter 6, Article 1, Section 1.3.4, Item 2.2.
The essential aspects of this description shall include identification and location of deficiencies within specific building systems including but not limited to the mechanical, plumbing, and electrical systems of the building and their respective components which fall within the scope of the nonstructural evaluation.
9. Often in hospital corridors the ceiling space is filled with pipes and conduits. Is it acceptable to create a secondary frame to “catch” the pipes to protect the exiting corridors instead of bracing all the pipes?
Though catching the pipes is important, it is not the primary issue. In addition to the potential as a falling hazard that the pipes may represent, it is also important to prevent escape of the pipes′ contents should the pipes break. Proper anchorage and bracing will reduce movement and shearing of pipes, and thus reduce the possibility of the escape of the contents. Therefore, the anchorage and bracing of pipes and conduits must meet the requirements of Chapter 16A, Part 2, 2022 California Building Code. Secondary framing is an option available for pipe bracing, but is dependent on site conditions.
10. Regarding air handlers that are functionally inadequate and have to be braced, do I have to replace them?
No, all that is required is that the air handlers be braced and anchored, not replaced.
11. If the intent of NPC 3 is to prevent loss of water from pipes in critical care areas, do we have to brace pipes from the central plant to the critical care areas? We infer the intent to prevent water loss from the valving option permitted. Can we only valve the pipes at the boundaries of critical care?
Pipes from the central plant supplying or passing through the areas specified in the NPC 3 category do not need to be braced outside the boundaries of those areas. However, equipment anywhere in the physical plant that services the NPC 3 specified areas shall be anchored and braced.
NPC 3 Exception 1 permits piping systems not be anchored and braced until 2030 (or 2024 based on Seismic Design Category F) provided that “an approved method of preventing release of the contents of the piping system in the event of a break is provided.” Valving the piping system is an acceptable method of preventing the escape of the pipe systems contents in the event of pipe breakage or shearing. The configuration of the valving layout depends on the layout of the piping within the NPC 3 specified areas. It should be noted that valving the pipes only at the boundaries may or may not prevent the release of pipe contents in those areas.
12. Could a policy be established which would clearly delineate the equipment within a hospital that would be affected by SB 1953?
No. As medical and other types of equipment vary from hospital to hospital, it is impractical to establish a policy with a definitive list of equipment which would be affected by SB 1953. The evaluation procedures and evaluation (appendix) questions delineate the conditions, equipment, systems, and components which fall under the general scope of the seismic evaluation.
13. In CAC Chapter 6 Article 11, the NPC process involves first a complete survey, then determining whether an HCAI permit exists, then making an NPC designation. This infers that in a code compliant structure, we have to do the whole survey even though it was built with full inspection. Can we not rely on an HCAI permit and inspection to designate the structure as compliant? Is it acceptable to look for permits first, and then survey the non-compliant areas?
The evaluator is free to perform the nonstructural evaluation in any manner desired. Hospital buildings constructed under a permit issued by HCAI are deemed to comply with the anchorage and bracing requirements of Title 24, with the exception of the fire sprinklers (unless constructed or retrofitted under NFPA 13, 1994 or subsequent edition). For other types of buildings, a review of the available drawings to determine the extent of the nonstructural bracing prior to conducting the site visit is very prudent. Aside from establishing the level of anchorage and bracing required to be expected, it will allow the evaluator to inventory components appearing on the drawings that should be braced. As a rule all major components that require bracing should be shown on the drawings. It is important to note that the NPC 3 evaluation is limited to those systems and components listed in the 1995 CBC, Part 2, Title 24, Table 16A-O.
All compliant buildings are not the same. Between 1973 and 1983, the enforcement of the code requirements for nonstructural elements, components and systems was inconsistent. The level of attention given to nonstructural bracing varied tremendously. This is substantiated by the nonstructural failures that occurred in various post-1973 hospitals as a result of the Northridge Earthquake.
In the late 1970′s and 1980′s some pre-1973 buildings had extensive remodels. The scope of these remodels can vary extensively, from cosmetic alterations to a complete gutting of the space, with reconstruction to current standards. It is not unusual to find braced and unbraced components next to each other in the same space. If the component or system was not modified during the remodel, then it was probably not seismically retrofitted. Only by inventorying the systems can the extent of the seismic bracing be definitively established.
14. Do hospital facilities need to meet the requirements of NPC 5 now?
For existing buildings, the milestone date for NPC 5 compliance is January 1, 2030 per 2022 California Administrative Code, Chapter 6, Table 11.1.
However, if a new seismically separate general acute care hospital building greater than 4000 square feet is constructed, it is required to be NPC 5 compliant per Section 1617A.1.40 of the 2022 California Building Code. Only the new building is required to be NPC 5 compliant and not the entire facility.
15. Is NPC 5 a campus-wide designation (like NPC 2) or a seismically separate building designation?
NPC 5 is a campus-wide designation with compliance expected in 2030, but new seismically separate buildings constructed to the 2010 or later California Building Codes are required to be NPC 5 compliant now. HCAI recommends planning to comply on a campus-wide basis with a phased approach to get NPC 5 compliance for a new building before it’s occupancy.
16. Is a hospital facility required to have storage tanks for 72 hours of water, sewage and liquid waste? The required tanks are too big and our site does not have the room for placement of such tanks.
NPC 5 refers to the ability of a hospital facility to support 72 hours of emergency operations. The California Plumbing Code has exceptions (see Sections 615.4 and 727.0 of the 2022 California Plumbing Code) that allow much smaller holding tanks where alternate arrangements have been made for delivery of water or transportable means for sewage and liquid waste disposal. Where such exceptions are used, the arrangements require approval by HCAI and the California Department of Public Health.
17. Does the NPC 5 requirement of 72 hours of water refer to potable water only? Is industrial water or (process) water to operate hospital utilities included in this storage requirement?
NPC 5 requirement refers to both potable water as well as industrial/process water to operate hospital utilities to support 72 hours of emergency operations:
For a seismically separate building that has licensed patient beds, a minimum of 150 gallons of potable water per licensed bed shall be provided (Section 615.4, 2022 California Plumbing Code) with additional industrial/process water to support 72 hours of emergency operation of the subject building. Also see exception in California Plumbing Code Section 615.4.1, for a seismic separate building that has no licensed patient beds, potable water and industrial/process water to support 72 hours of emergency operation of the subject building. A new Central Utility Plant must provide water for 72 hours of emergency operation for itself, any other new buildings but not for the existing buildings on the campus (The existing buildings will need to comply by 2030).
The amount of water required is determined from the facility’s emergency operations plan and an associated Water Conservation/Water Rationing Plan to provide for 72 hours of operation. The water conservation/water rationing plan must also be accepted by the California Department of Public Health licensing division. Whereas, there is a minimum volume of potable water per licensed bed, there is no minimum volume for industrial/process water in the California Plumbing Code. This volume is dependent on which utilities and systems the hospital facility intends to operate during an emergency. The Water Conservation/Water Rationing Plan must account for losses in the process water for closed loop heating and cooling systems.
See a planning guide titled “Emergency Water Supply Planning Guide for Hospitals and Health Care Facilities” published by DHHS, CDC and AWWA.
HCAI review of NPC 5 will be based on the volume of water required by the facility’s Water Conservation/Water Rationing Plan (as part of the facility’s emergency operations plan) as required by the California Plumbing Code.
18. Does the facility have to comply with Section 615.4.2 of the 2022 California Plumbing Code even when using the exception in Section 615.4.1?
Section 615.4.2 of the 2022 California Plumbing Code requires the emergency supply of water be provided with sufficient pressure using gravity, pressure tanks or booster pumps. If booster pumps are provided, they are required to be connected to the emergency power supply system.
Section 615.4.2 applies even when the exception of Section 615.4.1 of the California Plumbing Code is used, to ensure that the emergency supply of water is delivered to the end point of usage at sufficient pressure from the storage tank. The ability to dispense water to portable containers from the storage tank required in the exception of Section 615.4.1 of the California Plumbing Code is to be considered a measure of last resort.
19. Per Section 727 of the 2022 California Plumbing Code, can the facility store the sewage and liquid waste in a 5,000-gallon tank? Does this tank need to be connected to a sewage line?
Yes, holding tanks are required; however, there is no minimum size for the holding tank provided in Section 727, 2022 California Plumbing Code. The capacity shall be based on the Water Conservation/Water Rationing Plan required in Section 615.4.1.
The purpose of the holding tank is to permit 72 hours of continuing operation if the external sewer connection is severed. Thus, HCAI does not have any requirements for connection of the holding tank to the existing sewer line; however, such connections should be made with sufficient valves to isolate the external sewer lines.
20. Can we use bladder tanks to store sewage and waste water in the parking lot?
The exception to Section 727, 2022 California Plumbing Code permits use of leak-proof bags where adequate storage for such bags is provided where they comply with the appropriate local health and environmental authorities’ requirements, California Department of Public Health requirements for medical waste management AND requirement for location as well as enclosure.
HCAI takes no objection for use of the parking lot or any other location for storing these bags, if the storage location complies with the requirements of a lockable screen enclosure, floor, curb, drain connected to a sewer and supply of water as enumerated in this exception.
21. For NPC 5 evaluations, is the on-site emergency fuel storage requirement based on 96 hours or 72 hours? Are the fuel storage requirements based on fuel consumption of the generators at rated capacity or the actual load for the facility? Does the fuel storage requirement apply to N configuration only?
HCAI requires a minimum of 72 hours of on-site fuel supplyfor NPC 5 buildings (2025 CAC Chapter 6, Table 11.1; 2025 CBC Chapter 16A §1617A.1.40) that provide acute care operations. CMS—supported by Joint Commission guidance—requires compliance with the 2010 edition of NFPA 110 which requires that provisions be made to sustain the needs of the hospital for up to 96 hours when replenishment agreements are in place.
Accordingly, HCAI enforces 72 hours of on-site fuel storage with documented replenishment agreements to maintain alignment with current CMS and Joint Commission requirements.
2025 NFPA 110 §5.1.1.1 states that “on-site storage of an alternate energy source sufficient to allow full output of the EPSS to be delivered for the class specified shall be required.” For acute-care hospitals, the required class is 72 per 2025 CEC 517.31(H)(1). Therefore, the minimum on-site fuel storage capacity must provide 72 hours of fuel below the low-fuel sensor level to support fully loaded generator operation.
Note that the nominal tank capacity will necessarily exceed the calculated minimum 72-hour usable fuel volume.
As part of the NPC 5 evaluation report, the MEOR must include:
- Calculations demonstrating 72-hour usable fuel volume (from the fuel pickup point to the low-fuel sensor) for fully loaded generator(s).
- Nominal tank size and actual usable fuel volume.
- Low-fuel sensor set point and corresponding unusable fuel volume.
- For facilities with on-site storage greater than 72 hours but less than 96 hours, documentation of fuel replenishment agreements to meet CMS requirements must be provided to HCAI.
- For facilities with 96 hours or more of on-site storage, replenishment agreements are not required.
The “low fuel” point is defined as the level at which the main tank no longer contains sufficient fuel to meet the required full-load operating duration. The available fuel between the fuel suction tube and the low-fuel sensor must support 72 hours at full load fuel consumption rate.
CMS and the Joint Commission adopt the 2010 NFPA 110, which requires the tank to have a minimum capacity of 133% of the class. The 2025 NFPA 110 removes this 133% requirement for EES systems with Class > 24. However, facilities must still provide additional capacity above the low-fuel level to accommodate:
- Monthly generator maintenance runtime, and
- Any other systems drawing from the same tank with pickup points above the low-fuel level.
This additional capacity shall be coordinated with the vendor’s fuel supply delivery requirements.
N versus N+1 Configuration:
The minimum on-site fuel storage for an existing acute care hospital facility required to meet NPC 5 requirements shall be based on the actual load [“full-demand” on the Essential Electrical System (EES) per the 2025 CEC 517.31(H)(1). The full demand load of the existing EES should be calculated by following the method described in HCAI PIN 38 for level-one panel existing demand loads. The full-demand metered load taken at 125% should be used to determine the minimum number of generators required to meet or exceed the full-demand load at a particular site. Fuel sufficient to operate the minimum required generators at 100% for 72 hours shall be required. Note that for a N+1 configuration, fuel sufficient to operate only N generators is required.
Here is an example calculation to demonstrate these requirements.
Existing site has (2) 1500 kW/1875 kVA emergency generators. Facilities existing maximum demand load for the essential system is 1.4 MVA. [1.4 MVA x 1.25 = 1.75 MVA]
Therefore, the facility needs (1) 1500 kW/1875 kVA generator to meet site essential loads. Manufacturers listed fuel consumption for 1500 kW generators 100% loaded (full output) is 106.5 gal per hour.
- Nominal on-site fuel tank size = 12,000 gallons
- Available on-site fuel = 10,200 gallons (based on the lowest fuel supply pickup level and maximum fuel height level)
- Minimum on-site fuel supply requirement = 106.5 gal/hour * 72 hours = 7,668 gallons
- Low fuel sensor = 7,700 gallons
- CMS requirement = 106.5 gal/hour * 96 hours = 10,198 gallons
- Vendor requirement (24 hours duration between 72 to 96 hours) = 10,198 – 7,668 gallons = 2,530 gallons
22. What is NPC 3 upgrade requirements for GAC buildings that do not contain critical care spaces noted in 2022 California Administrative Code, Chapter 6, Article 11, Table 11.1?
The facility needs to submit a formal request for NPC 3 upgrade when a building does not contain any of the critical care spaces noted in the NPC 3 description. The NPC 3 upgrade request needs to provide a functional layout for all the areas in the building showing what the various areas are used for. Also, if equipment serving the critical care areas in other buildings is in the building in question, then a full NPC 3 upgrade would be required.
23. What are the NPC 4 and NPC 5 evaluation deadlines and requirements for noncompliant buildings?
Please see General Questions FAQ #9 for detailed instructions on submitting Removal of Acute Care Services (RACS) projects.
2025 California Administrative Code, Chapter 6, Article 1, Section 1.5.2.1
1.1. By January 1, 2024, the hospital owner shall submit to the Office a complete nonstructural evaluation up to NPC 4 or 4D and NPC 5, for each building.
For future RACS projects, the NPC 4/NPC 5 evaluation shall consist of a letter from the hospital (on hospital letterhead, signed by the Administrator/CEO) stating that BLD-xxxxx will be removed from acute care usage by January 1, 2030. Submit a Seismic Compliance Project application using the eServices Portal (eSP), and include this letter as a supporting document.
2025 California Administrative Code, Chapter 6, Article 1, Section 1.4.5
By January 1, 2026, the hospital owner shall submit to the office a compliance plan.
2025 California Administrative Code, Chapter 6, Article 1, Section 1.5.2.1
1.2. By March 1, 2026, the hospital owner shall submit to the Office construction documents for NPC 4 or 4D and NPC 5 compliance that are deemed ready for review by the Office, for each building that will continue to provide acute care services beyond January 1, 2030.
For future RACS projects, the facility will need to submit one or more RACs construction projects to meet the requirements of applying for Removal of Acute Care Services. If no construction is required for the removal of acute care services, then this step may be skipped.
2025 California Administrative Code, Chapter 6, Article 1, Section 1.5.2.1
1.3. By March 1, 2028, the hospital owner shall obtain a building permit to begin construction, for NPC 4 or 4D and NPC 5 compliance of each building that the owner intends to use as a general acute care hospital building after January 1, 2030. Hospitals not meeting the January 1, 2028 deadline set by this section shall not be issued a building permit for any noncompliant building except those required for seismic compliance in accordance with the California Administrative Code (Chapter 6), maintenance, and emergency repairs until the building permit required by this section is issued.
RACs construction project(s) shall obtain building permit(s) by January 1, 2028. After closure of these projects in compliance, a no construction RACs project shall be submitted to the Office, as per the eSP User Guide Applying for Removal of Acute Care Services, indicating whose jurisdiction the building will be in (local authority having jurisdiction or HCAI/OSHPD). Once that project is closed in compliance, submit a Seismic Compliance Project application using the eServices Portal (eSP) by January 1, 2030, to remove the building from the acute care building inventory.
Refer to PIN 80 and AB869 for eligibility and requirements related to the delay of the 2030 deadline. The delay application, if approved, does not change the deadlines listed above.
24. Can I upgrade from NPC 2 to NPC 4 or NPC 4D Level X directly? Or do I need to upgrade from NPC 2 to NPC 3, and then from NPC 3 to NPC 4 or Level 4D Level X?
The NPC upgrade can go directly from NPC 2 to NPC 4 or NPC 4D Level x.
25. Link to 1995 CBC Table 16A-O
26. Link to 1998 CBC Table 16B-O
27. Limits of Critical Care Areas
2022 California Administrative Code (CAC), Chapter 6, Article 1, Section 1.2 – CRITICAL CARE AREA means those special care units, intensive care units, coronary care units, angiography laboratories, cardiac catheterization laboratories, delivery rooms, emergency rooms, operating rooms, postoperative recovery rooms and similar areas in which patients are intended to be subjected to invasive procedures and connected to line-operated, electromedical devices.
In the case of a Surgical Services Department, for example, CBC 1224 calls for certain code required spaces such as staff locker rooms, nurse control office, etc. Because these rooms are required by code for a Surgical Services Department to function, must they also be considered Critical Care Areas? Or, do we take a strict definition of Critical Care Areas to include only spaces for patients?
The whole Surgical Services department would be the boundary of the NPC 3 critical care area.
28. Definition of an OSA Project
2022 California Administrative Code Chapter 6, Article 11, Sections 11.2.1.c.2; 11.2.2.d.2; 11.2.3.c.2; and 11.2.4.c.2 describes an OSA project as;
Reviewed and approved by the Department of General Services, Office of Architecture and Construction, Structural Safety Section. Drawings showing: a) the installation; b) bear an Office of Architecture and Construction, Structural Safety Section approval stamp; and c) a five-digit project number on the approval that begins with the “H” prefix,…
The leading “H” is counted as a digit in this description. The actual description is the OSA project number starts with an “H” followed by 4 digits.
29. How to demonstrate compliance of fire sprinklers constructed under various NFPA 13 editions: (revised 6/25/2026)
Use of 1994 NFPA 13 with the effective date of April 30, 1996 is considered compliant. For earlier construction, the scope of work is as follows:
With existing drawings:
1987, 1989, 1991 edition NFPA 13 Building Scope:
- Buildings where fire sprinklers are designed with 1991 edition NFPA 13: Design team required to add missing end-of- line restrains only.
- Buildings where fire sprinklers are designed with 1987 and 1989 edition NFPA 13: Design team to perform a site visit and verify original branch line bracing and end-of-line restrains exist. Design team required to add missing end of branch line restraints, missing longitudinal and lateral sway bracing for main and cross mains.
1985 edition and earlier NFPA 13 Building Scope:
- Buildings where fire sprinklers are designed with 1985 and earlier NFPA 13: All fire sprinkler piping shall be evaluated on site for as-built conditions. When existing construction documents are available, refer to FAQ#36 column titled “calculations and testing” based on the original permitting agency.
Verifying as-built conditions:
- For projects constructed under the 1987, 1989, and 1991 edition NFPA 13 if the design team observes either end of line restraints and main and cross main longitudinal and cross bracing, photo documentation will be sufficient to accept the as-built condition as part of an engineering report signed and stamped by the Structural Engineer of Record. However, the extent of site verification will need to be discussed, reviewed, and approved by the SCU.
- For projects constructed under or before the 1985 edition of NPFA 13, the design team shall observe end of line restraints and main and cross main longitudinal and cross bracing and submit an engineering report signed and stamped by the Structural Engineer of Record. However, the extent of site verification will need to be discussed, reviewed, and approved by the SCU.
No existing drawings or documentation:
For conditions where the existing as-built documents can’t be located, all fire sprinkler piping shall be evaluated on-site for as-built conditions. Submit an engineering report signed and stamped by the Structural Engineer of Record. However, the amount of site verification and photo documentation will need to be discussed, reviewed, and approved by the SCU.
30. For NPC 4D operational plan, 2022 CAC Chapter 6 Article 11.2.3.(f) states “..As-built plans, schematic, or other means showing the routing for all utilities serving the areas from their source to the areas they serve…”. There seems to be confusion on how much piping/conduits/ducts need to be shown. Are small pipes/conduits/ducts that are code exempt from bracing need to be shown on the schematic utility plan?
Although it is desirable to have of all exempt and non-exempt utility line drawings on hand, it is often not feasible. Therefore it is acceptable to show only non-exempt distribution systems in the NPC 4D operational plan .
31. Where can I find the California Department of Public Health Licensing and Certification All Facility letter (AFL 23-21)?
32. Are calculations for sizing of emergency generator fuel tanks for 72 hour minimum run time required to be submitted as part of the January 1, 2024, NPC 5 evaluation?
Yes. If the emergency generator fuel tanks are used for other purposes, that usage needs to be addressed in the calculations.
33. Can buildings and tunnels with an OSHPD approved NPC 4D Level 1, 2, or 3 rating supply services/systems and utilities to conforming buildings (SPC-3, -4, -4D, or -5) downstream?
2022 California Existing Building Code, Section 310A.1.1.1.1 does allow the use buildings or tunnels with an OSHPD approved NPC 4D Level 1, 2, or 3 rating to provide services/systems and utilities to conforming (SPC-3, -4, -4D, -5) buildings downstream of the NPC 4D Level 1, 2, or 3 building or tunnel. However, as part of the approval of the NPC 4D Level 1, 2, or 3 upgrade for these buildings or tunnels, the NPC 4D Operational Plan required by 2022 California Administrative Code, Chapter 6, Article 11, Section 11.2.3.f, shall address showing how for all critical care areas in the downstream buildings the facility will repair nonstructural damage and bring systems and services back on line for the downstream critical care areas, or provide downstream critical care areas in an alternative manner to accommodate continuation of critical care operations.
34. When citing a project to show a piece of equipment anchorage compliance, can I only cite the project, or do I need to cite the detail number, sheet number, and project number?
Citing the project number is adequate to show anchorage compliance.
35. If the NPC 5 submittal is part of a package submitted by a licensed design professional, does it need to be sealed and signed by a licensed design professional?
If the NPC 5 report is submitted by a licensed design professional, it needs to be signed and sealed by a licensed architect or mechanical engineer.
36. What are the NPC requirements for buildings from different eras?
The table below lists the requirement for NPC 3, 4 and 4D7.
| Approximate Year | Original Permitting Agency2 | Self Declaration6 | Equipment Inventory1 | Distribution Systems Evaluation | Fire Sprinkler Evaluation | Calculations and Testing |
|---|---|---|---|---|---|---|
| Prior to 1973 | Local | NA | R | R | R | Yes5 |
| 1973 to 1982 | OSA2 | NA | R | R | R | Maybe4 |
| 1982 to 1994 (1994 NFPA-13) | OSHPD3 | Required | NR | NR | See FAQ #29 | NR |
| 1994 (1994 NFPA-13) to Present | OSHPD3 | Required | NR | NR | NR | NR |
NA = Not Allowed
NR = Not Required
1 Not required for complete gut and remodel (floor to floor) projects done under HCAI. Partial remodel requires equipment inventory
2 Refers to project numbers starting one letters and four number (example H1001)
3 Refers to project numbers starting two letters and six numbers (example HL860034)
4 Field verification required for general conformance (testing maybe required)
5 Refer to 2022 CAC Chapter 6 Table 11.1 for force level (CBC 1998)
6 For NPC 4 self-declaration refer to 2022 CAC Chapter 6 Article 11 item 11.01 item 2. Self-declaration does not apply to other NPC categories.
7 NPC 4D requires operational plan as part of evaluation per 2022 CAC Chapter 6 Article 11 item 11.2.3
37. What are the testing requirements for tension and shear for existing anchors?
Demand, capacity, and testing requirements are listed under 2022 CAC Chapter 6 Article 11 §11.3 and clarified below for NPC-3, 4, and 4D:
- Tension and shear demands shall be calculated per 1998 CBC §1630B as listed under 2022 CAC Chapter 6, Article 11, §11.3.
- Tension and shear capacity for cast-in-place anchors shall be per Table 19B-E of the 1998 CBC. The tension and shear capacity for post-installed anchor tension and shear capacity is allowed to be per the ICC ER report matching the anchor manufacturer and code cycle at the time of installation.
- Testing:
- Tension: Refer to §11.3.1 and §11.3.2 for testing frequency, demand (3*tension), usage type (equipment versus distribution system), and permitted exceptions.
- Shear: Shear testing or tension testing is not required when analysis indicates only shear demand (no tension).
- Alternate testing criteria are permitted per §11.3.4.
38. If the design professional doing an NPC 4 reconciliation report determines that an area has not been constructed under an OSA or OSHPD project, but planned to be fully renovated later, can they note the renovation as future deficiency mitigation through a construction project?
The NPC 4 upgrade and reconciliation report needs to note the areas that are deficient and compliant for the January 1, 2024 submittal deadline. The renovation project will need to be submitted to the Office by January 1, 2026; with a building permit issued by January 1, 2028; and construction being completed by January 1, 2030.
39. What is the minimum number of elevators required by NPC 4D Level 2 and NPC 4D Level 3 upgrades?
There shall be a minimum of one elevator selected to provide service to patient, surgical, obstetrical, and ground floors during interruption of normal power. The selected elevator shall be capable of carrying a gurney. The selected elevators do not need to be in the building requesting the NPC 4D Level 2 or Level 3 upgrade, but shall be accessible on the patient, surgical, obstetrical, and ground floors and be reasonably close to the building in question.
40. Can the first NPC 3 exception in the 2022 California Administrative Code, Chapter 6, Article 11, Table 11.1 be used for NPC 4 evaluations?
2022 California Administrative Code, Chapter 6, Article 11, Table 11.1
“Lateral bracing of suspended ceiling systems may be omitted in rooms with a floor area less than 300 square feet, provided the room is not an intensive care or coronary care unit patient room, angiography laboratory, cardiac catheterization laboratory, delivery room, operating room or post-operative recovery room. For rooms with a floor area greater than 300 square feet, OSHPD pre-approved standard details may be used.”
No, this exception cannot be used for NPC 4 evaluations. However, the use of all exceptions in 2022 California Building Code is permissible for NPC 4 ceiling evaluations
41. When is verification of flex joints, or alternate means of handling differential movement of pipes, conduits, ducts at seismic separation joints between two buildings required?
[For NPC 4, NPC 4D Level 2, NPC 4D Level 3] Please verify if utilities, services, and systems crossing seismic joints can accommodate the relative building displacements or have a flex joint per the following table. Alternatively, where the building does not meet this criteria, or the seismic utility flex-joint survey is not performed, the design professional of record shall state the following sentence in the report: “The building might not be functional after an earthquake due to failure in utilities between adjacent buildings”. The following table clarifies where the survey is required.
Utility flex-joint survey requirement table:
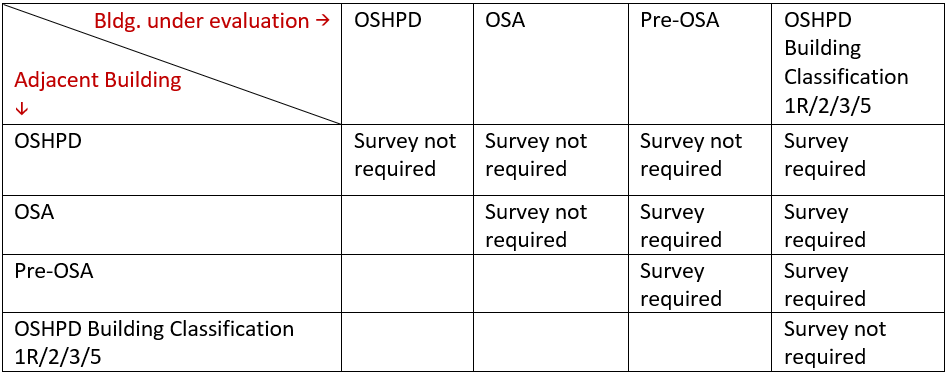
42. Can the entire facility be upgraded to NPC-4D Level 1?
No, NPC 4D Level 1 is for a building without critical care services or building that the critical care functionality can be provided in an alternative manner in another compliant building within the same facility. All buildings in the facility cannot be NPC 4D Level 1 as in the event of earthquake repairs are often not be feasible, and contractors/vendors may not be available, and therefore the facility may end up shutting down, not providing the required acute care services. The evacuation is a last resort option, not a design target.
43. Can a Central Utility Plant (CUP) building, cooling tower or equipment yard be upgraded to NPC-4D Level 1 or 2 or 3?
No, these buildings can only be upgraded to NPC-4 level of compliance. These buildings serve the entire facility and therefore should be in operation after an earthquake.
44. The requirement for piping suspended by individual hangers 12” or less in length from top of pipe to bottom of support has changed in CBC 2016 and CBC 2019. Is it acceptable to use previous CBC codes for the exception?
The exception from 1998 code or later codes but not a combination thereof, shall be considered acceptable to satisfy the requirements of NPC reclassification.
45. Are the NPC-3 exception in table 11.1 of California Administrative Code (CAC) applicable for NPC-4D Level1, Level 2, level3 or NPC-4 reclassification.
- NPC-4D Level1: All the NPC-3 exceptions in table 11.1 of California Administrative Code (CAC) are applicable to NPC-4D Level1.
- NPC-4D Level2: Seismic restraints from source to NPC-3 areas (including within the NPC-3 areas) shall be provided for cable trays, conduit, HVAC ducting and piping systems. The exception for NPC-3 cable trays, conduit, HVAC ducting and piping systems is not applicable. As indicated in NPC-4D L2/L3 requirement, elevator(s) selected to provide service to patient, surgical, obstetrical and ground floors during interruption of normal power needed, shall meet the structural requirements of Part 2, Title 24. The remaining NPC-3 exceptions in table 11.1 of California Administrative Code (CAC) are still applicable.
- NPC-4D Level3: Same as NPC-4D level 2 that applies to level 3 areas.
- NPC-4: None of the NPC-3 exception in table 11.1 of California Administrative Code (CAC) are applicable to NPC-4 reclassification.
46. For buildings retrofitted to meet NPC-3R standards, can a consultant verify the adequacy of the anchorage through field observation?
No, the anchorage designed under NPC-3R standards was calculated with an importance factor (I) of 1.0, while NPC-3 requires an importance factor of 1.5. Installations or retrofits designed to meet NPC-3R standards must be evaluated to ensure they meet the anchorage and bracing requirements of the California Building Code for NPC-3. If the existing anchorage is insufficient to meet the forces required for NPC-3 compliance, a retrofit is necessary. See California administrative code section 11.2.3 item c.1.
47. California Administrative Code requires an executive summary per Chapter 6, Section 1.3.4. Is there a template we can use?
NPC 4: The below template is recommended to be included in NPC 4 building evaluation reports as required per 2022 CAC, Chapter 6, Section 1.3.4. This will streamline the NPC Upgrade process by summarizing the nonstructural deficiencies about the building and the scope of retrofit work to be done. Reference the section numbers within the report describing the details of scope of work.

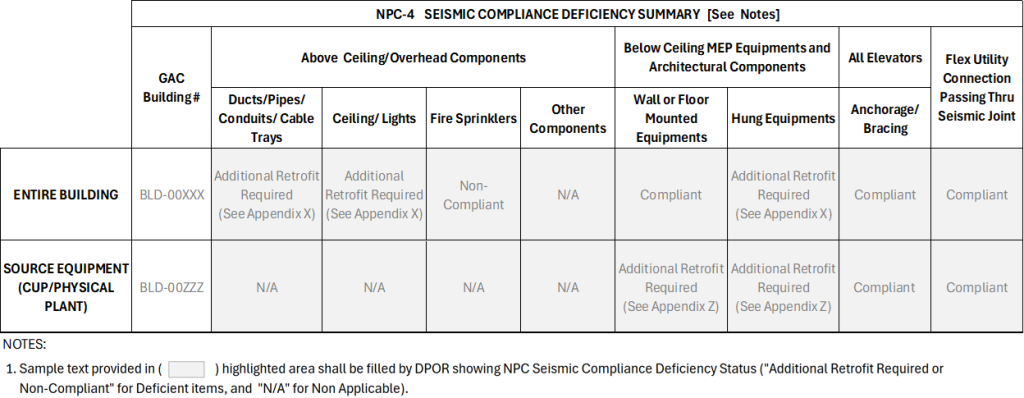
NPC 4D Level 1: The below template is recommended to be included in NPC 4D Level 1 building evaluation reports as required per 2022 CAC, Chapter 6, Section 1.3.4. This will streamline the NPC Upgrade process by summarizing the nonstructural deficiencies for the building and the scope of retrofit work to be done. Reference the section numbers within the report describing the details of scope of work.

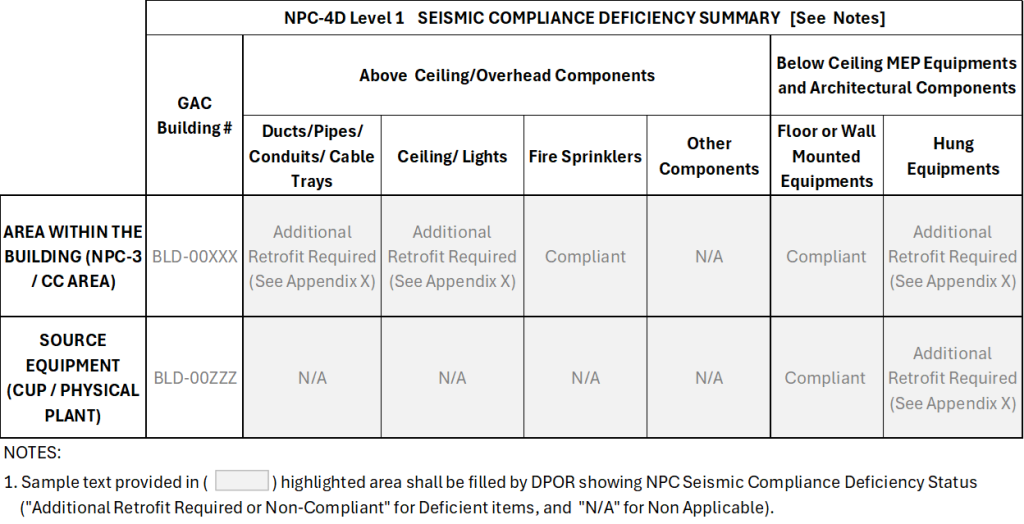
NPC 4D Level 2 or Level 3: The below table template is recommended to be included in NPC 4D Level 2 or Level 3 building evaluation reports as required per 2022 CAC, Chapter 6, Section 1.3.4. This will streamline the NPC Upgrade process by summarizing the nonstructural deficiencies for the building and the scope of retrofit work to be done. Reference the section numbers within the report describing the details of scope of work.

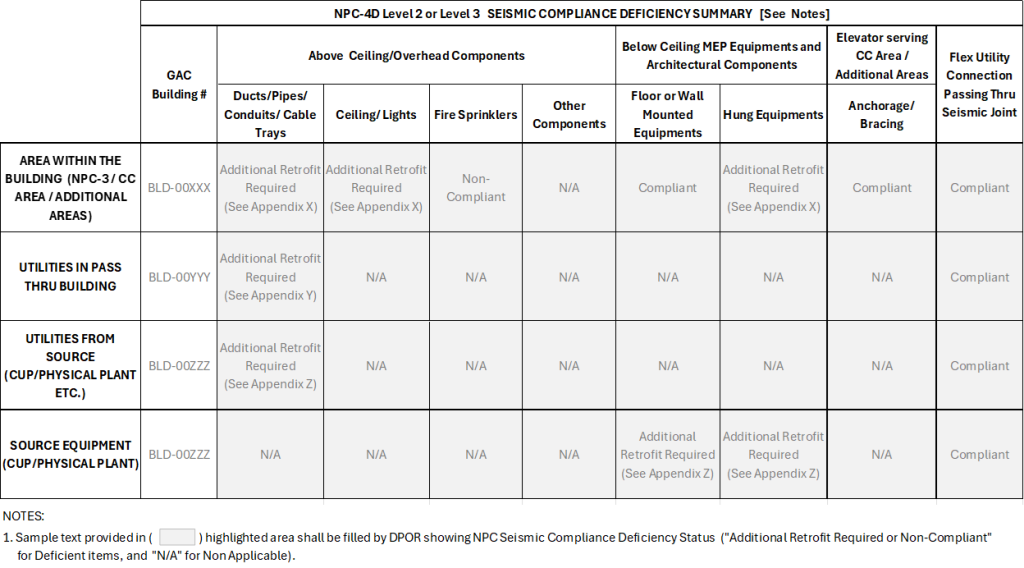
Here is the link to the NPC 4/4D executive summary templates
48. The operational plans shall have an executive summary per 2022 California Administrative Code, Chapter 6, Section 11.2.3.f. Is there a template we can use?
In addition to the nine items listed under 2022 CAC, Chapter 6, Section 11.2.3.f, the following executive summary template shall be included in NPC-4D Level 1, Level 2 or Level 3 building evaluation reports. This will streamline the NPC Upgrade process by summarizing the functional status of services to the building for the operational plan. (Revised 05/13/25)
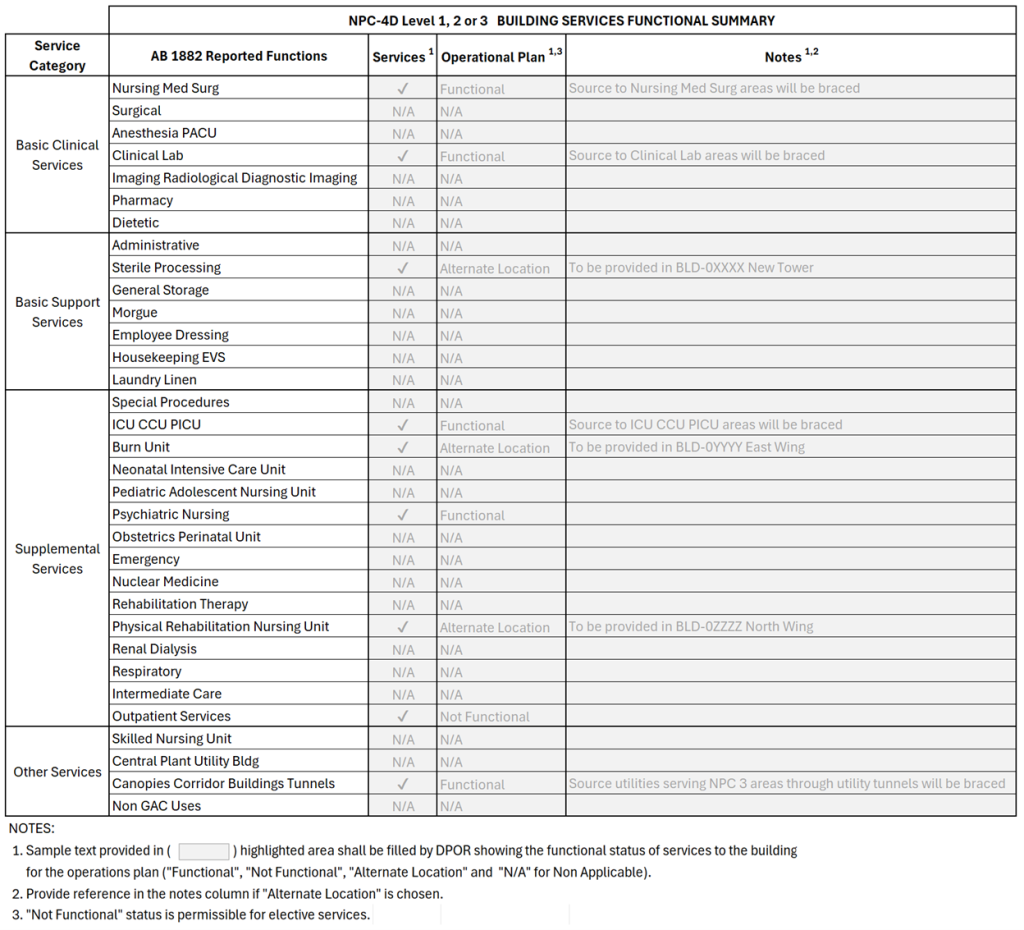
49. What steps are required to reclassify NPC-2 buildings constructed under OSHPD permit to NPC-4D Level 1, 2, or 3?
It is suggested to reclassify these buildings to NPC-4 through self-certification letter (per CAC section 11.01 item 2.2) and retrofitting the fire sprinkler in entire building per NFPA 1994 edition, or subsequent applicable standards, however if NPC-4D reclassification is pursued following step are required.
- NPC-4D Level 1:
- Retrofitting the fire sprinkler within NPC-3 areas per NFPA 1994 edition, or subsequent applicable standards
- Retrofitting source equipment that services the NPC-3 areas of the building
- Provide operational plan
- NPC-4D Level 2:
- Retrofitting the fire sprinkler within NPC-3 areas and from source to NPC-3 areas per NFPA 1994 edition, or subsequent applicable standards
- Retrofitting source equipment that services the NPC-3 critical areas of the building
- Retrofitting all services and utilities from the source to NPC-3 areas necessary to accommodate continuation of operations after an event
- Provide operational plan
- NPC-4D Level 3: includes Level 2, and all systems and equipment are anchored and braced so that additional services, as determined by the hospital in its Operational Plan are functional and available to the public after a seismic event
Providing inventory or retrofit of equipment and utilities (except fire sprinkler) within the OSHPD building is not needed if a written statement by the hospital owner is submitted to OSHPD certifying the a) The building was designed and constructed under a building permit issued by OSHPD; b) All subsequent repairs, remodels, additions and alterations were performed under a permit issued by OSHPD. The OSHPD project number associated with original construction shall be closed in compliance.
50. Certain functions of the NPC-3 area in the building can be provided through alternative means, while others are exclusive to this building. Does this building meet the criteria for NPC-4D Level 1 compliance?
Per 2022 California Administrative Code Section 11.2.3 for minimum compliance including Level 1, the building must ensure the continuity of critical care operations. For areas where functions can be provided through alternative means, no further action is required under Level 1 other than upgrading the NPC 3 areas and equipment serving NPC 3 areas in other building to meet the NPC 3 requirements. Services and utilities must be retrofitted, extending from their source to the NPC-3 areas where the service is exclusive to the building and no alternative means are available. If these requirements, along with all other NPC-4D Level 1 criteria, are met, the building will be eligible for NPC-4D Level 1 compliance.
51. Is an end-of-line restraint required for fire sprinkler piping under NFPA 13 (1994 edition) when there is no ceiling?
End-of-line restraints are typically intended to mitigate the risk of sprinkler heads being sheared off at the ceiling level during a seismic event. When no ceiling is present at the sprinkler elevation, this specific risk does not exist. Therefore, the requirement for an end-of-line restraint may be waived, provided no other conditions in NFPA 13 necessitate it.
52. Could you clarify NPC-3 areas in “AB 1882 Building Reported Functions” list?
See below template where the NPC-3 areas are gray highlighted, also within the gray highlight red text implies Critical Care Areas.
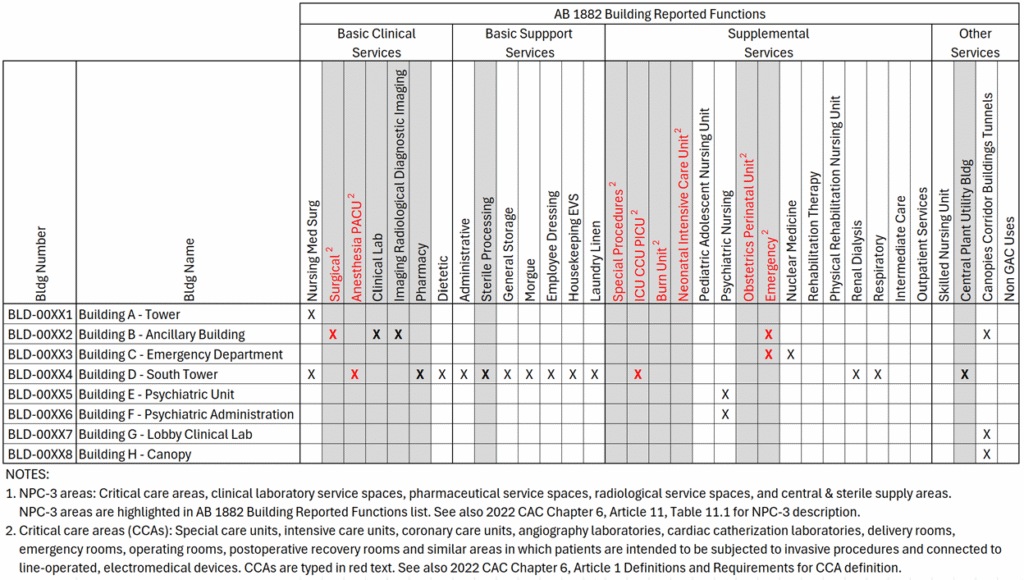
53. What are the NPC upgrade requirements for suspended ceiling?
For OSA and pre-OSA buildings, suspended ceilings greater than 144 sq. ft. shall be evaluated and retrofitted to the 1998 CBC (i.e. have a minimum of four (4) #12-gauge wires secured to the main runner within 2″ of the cross runner with a compression strut. These shall be at 12’0” maximum spacing and not more than 6’0” from each wall unless otherwise specified in the 1998 or later building code.) Clearance/Gap between the ceiling and walls may not be present in the existing condition; however, providing clearance/gap is not required. For retrofit or replacement, OSHPD pre-approved standard details may be used.
Example:
- For OSA buildings with construction documents, if the SEOR verifies that the onsite condition is in reasonable conformance with the available construction documents, no further action is required. Refer 2022 CAC Chapter 6 §11.2.3.c.2
- Per CAC Table 11.1 NPC 3 Nonstructural components exception 1, lateral bracing of suspended ceiling systems may be omitted in rooms with a floor area less than 300 square feet, provided the room is not an intensive care or coronary care unit patient room, angiography laboratory, cardiac catheterization laboratory, delivery room, operating room or post-operative recovery room. This exception only applies to NPC 4D L1, L2 or L3 upgrades (not NPC 4)
54. What target NPC 4D Level is to be used for buildings that do not have NPC-3 areas?
The building is not eligible for an upgrade to NPC 4D Level 2. Because the building does not have any NPC-3 areas, there is no utilities and services from source to the NPC-3 areas of this building to be retrofitted. Consequently, the building needs to have the desired NPC 4D Level set to Level 1 (or NPC 4). If the building contains source equipment serving NPC 3 areas in other buildings, the operational plan needs to note that there is source equipment in this building serving other buildings and identify those buildings.
55. What is the required scope for fire sprinkler bracing work associated with NPC 4D L2 or L3 projects?
- Are end-of-line braces required in areas that are not designated as critical care?
- Are main line bracing for fire sprinkler lines that do not serve critical care areas required?
- For multi-story hospitals, are shut-off valves required for upper floors that do not include critical care areas? (Critical care areas are only on 1st floor.)
The scope of work for fire sprinkler longitudinal, sway bracing, and end of line restraints for NPC 4D L2 and L3 projects are limited to the critical care areas and the source fire sprinkler lines that serve those critical care areas.
- No, end of line restraints are not required in areas that are not within critical care areas for NPC 4D L2/L3.
- No, main line bracing for fire protection is not required if the mains do not serve the critical care areas for NPC 4D L2/L3.
- It is recommended to isolate the sprinkler system that feeds the critical care areas through shut off valves. This would minimize the effect of damage coming from unbraced areas but shut off valves are not required by code.
Skilled Nursing Facility (SNF)/Acute Psychiatric Facility
1. Do Skilled Nursing Facility buildings have to meet the requirements of SB 1953?
Skilled Nursing Facility buildings (SNFs) which are licensed under 1250 (c) of the Health and Safety Code do not have to meet the requirements of SB 1953. Also precluded are hospital buildings that are licensed under Section 1250 (a), General Acute Care, but provide skilled nursing services only. For additional information, refer to the response to Question #3 below.
2. What are the SB 1953 requirements when a Skilled Nursing Facility (SNF) is on the third floor of a General Acute Care (GAC) building?
The entire building is subject to the SPC requirements. With respect to the NPC requirements, the SNF area would not be considered “critical care area” under the NPC 3 category for compliance, but it will be subject to the NPC 4 and NPC 4D requirements for compliance.
3. My SNF building is under GAC license but it is a separate building on the campus. Does SB 1953 require this building to be evaluated?
The Seismic Evaluation Procedures and Compliance Plan Regulations were developed by HCAI specifically for implementation by GAC licensed hospital buildings in furtherance of the Alfred E. Alquist of Hospital Facilities Seismic Safety Act of 1983. These regulations require GAC licensed hospitals to perform seismic evaluations on their respective facilities and for mitigation of substandard structural and nonstructural conditions by the seismic retrofit (compliance) plan.
In the 2022 California Administrative Code, Chapter 6, Section 1.2, Definitions, the term “General Acute Care Hospital” is defined. It states in part the following:
“…a hospital building as defined in Section 129725 of the Health and Safety Code and also licensed pursuant to Section 1250 (a) of the Health and Safety Code…(but) It also precludes hospital buildings that may be licensed under the above mentioned code sections, but provide skilled nursing services only.”
Therefore, a building which contains no GAC licensed beds or services but is used only for SNF beds and services is not subject to the requirements of SB 1953 even though it is under the GAC license. However, the building must be “freestanding and separate” in accordance with the conditions set forth in #HSC-129725, revised August 20, 1996. For additional information, refer to Question #4 below.
4. If all the GAC beds are moved into one building and all the SNF beds are moved into and/or remain in another building, is the building containing the SNF beds subject to the requirements of SB 1953?
No. Even if the SNF beds are listed on the general acute care license, this building is not subject to SB 1953. It is not a hospital building within the meaning of Section 130005 (k) of the Health and Safety Code. See also 2022 California Administrative Code, Chapter 6, Part 1, Article 1, Section 1.2, Definitions – General Acute Care Hospital. This section explicitly excludes hospital buildings that provide skilled nursing services only. However, this building must be physically separate from the building housing GAC services or be separated by a seismic joint. This answer also applies to existing, separate buildings listed on the general acute care license that exclusively contain SNF beds.
Facilities should be aware of the possible Medi-Cal reimbursement consequences of a general acute care hospital providing SNF services in a separate building. Reference should be made to Health and Safety Code Sections 1250.8 and 1254 relating to separate licenses for “separate freestanding facilities” providing SNF services.
Facilities should also be aware that Department of Public Health licensing approval is required before beds or space approved for one use may be used for or converted to another use.
If a new, separate SNF license is required, facilities should consult with HCAI and the Department of Public Health licensing to discuss the means by which they will demonstrate compliance with Title 24 requirements (including structural) for SNF′s. The facility, of course, may request the utilization of alternate means and methods found in Chapter 1, Part 2, Title 24.
Facilities should also be aware of §72205 of Title 22 which requires that “The licensee shall maintain the skilled nursing facility in a safe structural condition. If the Department determines in a written report submitted to the licensee that an evaluation of the structural condition of a skilled nursing facility building is necessary, the licensee may be required to submit a report by a licensed structural engineer which shall establish a basis for elimination or correcting the structural conditions which may be hazardous to occupants. The licensee shall eliminate or correct any hazardous conditions.”
5. Are acute psychiatric (or skilled nursing) facilities exempt from seismic retrofit requirements?
Seismic retrofit requirements apply to General Acute Care Hospital buildings (as defined in the 2022 California Administrative Code Chapter 6), therefore, buildings, including SPC and/or free-standing buildings, providing only skilled nursing or acute psychiatric services are exempt.
Conversion of General Acute Care Hospital buildings for acute psychiatric or skilled nursing uses can be complex especially if the subject building is located in a facility that also provides general acute care services in other buildings at the same site. It is recommended that a meeting with the regional supervisor of the Building Safety Section of HCAI/OSHPD be arranged to discuss all possible issues related to the conversion.
Chapter 6 of the 2022 California Administrative Code
GENERAL ACUTE CARE HOSPITAL as used in Chapter 6, Part 1 means a hospital building as defined in Section 129725 of the Health and Safety Code and that is also licensed pursuant to subdivision (a) of Section 1250 of the Health and Safety Code, but does not include these buildings if the beds licensed pursuant to subdivision (a) of Section 1250 of the Health and Safety Code, as of January 1, 1995, comprise 10 percent or less of the total licensed beds of the total physical plant, and does not include facilities owned or operated, or both, by the Department of Corrections. It also precludes hospital buildings that may be licensed under the above mentioned code sections, but provide skilled nursing or acute psychiatric services only.
Compliance Plan
1. Do I need to submit a compliance plan for a facility that is already 2030 Compliant for all buildings?
Per PIN 80, an owner of a hospital building not in compliance with Health and Safety Code Section 130065 shall submit for review and approval a revised compliance plan to the Department no later than January 1, 2026. Facilities that are in compliance with Health and Safety Code Section 130065 (2030 Compliant for all GAC buildings at the facility) do not need to submit a compliance plan.
2. How do I submit a Compliance Plan and what is required?
1. Compliance plans should be submitted using the eServices Portal (eSP).
- For step-by-step instructions please download User Guide 21 – Application for Seismic Compliance Plan.
2. When submitting a Compliance Plan in eSP, include the following information:
- Compliance Method:
- The Building Number, Building Name, Current SPC Rating, and Current NPC rating are pre-populated at the time of compliance plan project creation.
- Compliance Type – Select the appropriate value from the drop-down list.
- Narrative – Provide an explanation for the Compliance Type choice.
- Seismic Compliance Related Project Numbers – List project numbers separated by a semicolon.
- HCAI Note – Is a read-only field and will be completed by HCAI staff, if applicable.
- Building Milestones:
- Milestone Type – See sample template (Updated 12/10/25 – See changes to Example #7) for suggested Milestone Type drop-down values.
- Description – Provide an explanation for the Milestone Type choice.
- Critical Milestones – At least one milestone shall be selected as a critical milestone for each significant building, such as larger general acute care buildings, e.g. main hospitals, patient wings, central utility plants, D&T buildings, etc.
- Critical milestones can be skipped for minor buildings such as canopies, tunnels, sheds, equipment yards, or buildings that are not as important/significant relative to the rest.
- Regular milestones are still required for all buildings.
- Completion Date – Provide the milestone completion date. If the final completion date is beyond 1/1/2030, and if the facility does not have an approved extension*, HCAI will remark the compliance plan. This remarked compliance plan will be published on HCAI website. *Eligible facilities may apply for the AB 869 delay in compliance to extend the 1/1/2030 deadline, but if it is not granted, or the facility chooses not to apply, HCAI cannot approve compliance plans with completion dates beyond 1/1/2030.
- Status – Indicate if milestone is “Not Started”, “In Progress”, or “Completed”.
- Related Project Numbers – List OSHPD project number(s) related to the milestone. Separate project numbers by a semicolon. Building permit project numbers need not be entered. Preliminary project numbers are acceptable but need to be updated to the final project number when it is submitted.
- HCAI Note / HCAI Determination / Notes – These fields are read-only and will be completed by HCAI staff, if needed.
3. How do I submit an update to an existing Compliance Plan?
Updates to Building Milestone Status and Related Project Number can be made by emailing SeismicComplianceUnit@hcai.ca.gov. Indicate the building number, milestone, and provide the revised Status and/or Related Project Number(s).
Updates for all other items not noted above require the submittal of an amended Compliance Plan using the eServices Portal (eSP). For step-by-step instructions, see Chapter 5 – Amending an Application for Seismic Compliance Plan of the User Guide 21 – Application for Seismic Compliance Plan.
Hospital Services Reporting (AB 1882)
1. Who must report yearly under AB 1882?
All operational hospitals licensed as general acute hospitals or that have any general acute care category licensed beds that are subject to SB 1953 requirements. This means acute rehabilitation hospitals, surgical hospitals, etc., are subject to the reporting requirements. The owner of an acute care inpatient hospital that includes a general acute care building that is not SPC 3/NPC 5, SPC 4D/NPC 5, SPC 4/NPC 5, or SPC 5/NPC 5 shall provide an annual status update on the Structural Performance Category ratings of the buildings and the services provided in each hospital building on the hospital campus.
2. How do I do the required reporting?
The reporting needs to submitted online through eServices Portal (eSP). See eSP User Guide Hospital Services Reporting for instructions.
3. What documents are required for AB 1882 service reporting application?
Please follow the eSP User Guide Hospital Services Reporting. No additional documents are required.
4. What should be reported when the facility NPC/SPC ratings have “s” letters, such as SPC 5s, NPC 4s?
An “s” designation is a reported SPC/NPC rating to HCAI/OSHPD, not an approved rating. This “s” designation typically indicates that there is some missing documentation that is required to be provided. Please email the Seismic Compliance Unit (SCU) for instructions to clear “s” designation.
5. When filling out the services in the eSP application website, can I leave a blank for service type for a building?
No, all buildings need at least one service selected. If the building doesn’t contain any of the acute care services, select ‘Non-GAC Uses’ and enter a brief description of the building service(s).
6. What if my facility no longer has any acute care functions, but is licensed as a General Acute Hospital?
Contact CDPH L&C to see if the facility needs to be relicensed to reflect the current usage. Once the facility is relicensed as something other than a General Acute Care hospital, please email the Seismic Compliance Unit (SCU) a scanned copy of the license and the record will be updated to exempt the AB 1882 reporting requirement.
7. What if I need to add a GAC building to the inventory?
Submit a Seismic Compliance Project application using the eServices Portal (eSP) to add a building to the OSHPD building inventory. Following the creation of the new building number, AB 1882 reporting of the services for the added building is required.
8. What if I need to remove a GAC building from the inventory?
Submit a Seismic Compliance Project application using the eServices Portal (eSP) explaining why the building should be removed from the building inventory. Reasons include demolition, reclassification as an OSHPD 1R, building returned to the local authority having jurisdiction, etc. The AB 1882 services list will be updated following the removal of the building.
Hospital Signage (AB 1882)
1. PIN 75 states the following: “The proposed location and the content of the notice are required to be accepted by the department through a construction project submittal.” Is an Amended Construction Document (ACD) or a new project acceptable to submit for posting?
Please submit an application with a specific record type (GACSIGN) using the eServices Portal (eSP). Please follow the eSP User Guide Hospital Signage Reporting for the step-by-step application process.
2. What documents are required for the signage application?
Please follow the eSP User Guide Hospital Signage Reporting. A floor plan showing the signage locations and the signage page selected and filled in from PIN 75 are required to be uploaded as part of the AB 1882 signage application.
3. Is only one notice needed for each non-compliant structure?
The law requires posting in any lobby or waiting area generally accessible to patients. The department may agree with a fewer number of posting locations depending on the floor(s) layout and use of space. Please submit an application with proposed posting locations for the department’s review and approval.
4. Can this be done as part of another ongoing project on the site?
No. Please submit a new AB 1882 signage application using eSP.
5. There are general acute care buildings without lobby or waiting areas, would posting still be required?
If there is no lobby or waiting area, the department will review the location of the posting on a case-by-case basis. AB 1882 posting is not required for equipment yards, tunnels, canopies, cooling towers, or emergency generator enclosures.
6. Are these signs expected to be printed pieces of paper? What about signage to wall connection detail?
There is no required material type for the signage. The signage should be protected from damage and securely adhered or hung on the wall.
7. Is it sufficient to provide a general location, such as pointing to the approximate area on a floor plan, or does the exact location need to specified?
Pointing to the approximate area on a floor plan is acceptable. The installed signage is required to be verified and accepted by HCAI field staff.
8. Will the HCAI regions be reviewing these AB 1882 projects, or will they go through the Seismic Compliance Unit (SCU)?
Review and approval will be done by the corresponding region or field staff.
9. Do we need to complete project kick-offs with the field staff? District Structural Engineer (DSE), Fire Life Safety Officer (FLSO), and Compliance Officer (CO)?
No.
10. Do we need an Inspector of Record (IOR), Testing Inspection Observation Program (TIO), or Verified Compliance Report (VCR) by the Design Professional of Record (DPOR)?
No.
11. Can the sign be moved at a later date?
For revised location, please submit a new AB 1882 signage application using eSP.
12. Is a version of the sign for the visually impaired required?
Braille signage is not required.
13. Can the facility provide supplemental information to the posting?
No supplemental information on the posting will be allowed. However, additional informational postings around the signage that does not interfere with the AB 1882 signage posting is allowed.
14. The statement says no deviation from the notice format. Assuming that the format remains as is, can the statement be adjusted?
The statement, the size, or the format cannot be revised.
15. Is the signage requirement in Section 130065 applicable only to the first floor, or does it apply to all floors including the basement in multi-story buildings?
The signage requirement in Section 130065 applies to all floors in multi-story buildings, including the basement. This is because the section states that signs must be posted in “any lobby or waiting area generally accessible to patients or the public.” Therefore, all floor plans, including the basement, must be submitted with the locations of posted signage clearly marked. In the absence of lobby or waiting room place the signage in front of elevator/stair exit or in corridor. A minimum of one signage per floor is required.
16. Is signage required for a building that is not open to the public or does not see patients or provides no general acute care services?
Yes, provide at least one signage for OSHPD 1 building at each floor.
17. Is signage required for OSHPD 1R or OSHPD 2 or OSHPD 5 buildings?
Signage is not required for OSHPD 1R or OSHPD 2 or OSHPD 5 buildings.
18. If the building SPC or NPC rating changes, would revised signage be required?
Yes.
19. Does a GACSIGN project need to be submitted every year once the initial sign project has been accepted and the signs installed?
No, updated GACSIGN projects need only be submitted when the SPC or NPC rating of the building is changed and that change is approved by the Seismic Compliance Unit. If the floor plan(s) remains the same as the previous GACSIGN submittal floor plan(s), then the floor plan(s) previously submitted may be used and the updated signage graphics submitted.
20. What should be done with previously approved signs when a building is reclassified as an OSHPD 1R building?
It is acceptable to remove the signs after the OSHPD 1R reclassification has been approved by the Office.